CME
Physicians: Maximum of 0.75 AMA PRA Category 1 Credit™
Released: September 09, 2025
Expiration: March 08, 2026
Introduction
In this module, Eytan Stein, MD, and Eunice Wang, MD, provide an overview of the latest evidence on menin inhibitors for patients with acute leukemias and NPM1 mutations (mNPM1) or KMT2A rearrangements (KMT2Ar).
The key points discussed in this module are illustrated with thumbnails from the accompanying downloadable PowerPoint slideset, which can be downloaded by clicking on any of the slide thumbnails in the module alongside the expert commentary.
Please note that Clinical Care Options plans to measure the educational impact of this activity. Some questions are asked twice: once at the beginning of the activity, and once again after the discussion that informs the best choice. Your responses will be aggregated for analysis, and your individual responses will not be shared. Thank you in advance for helping us assess the impact of this education.
Before continuing with this educational activity, please take a moment to answer the following questions.
Incidence of MLLr and NPM1-Mutant Acute Leukemia
Eytan Stein, MD:
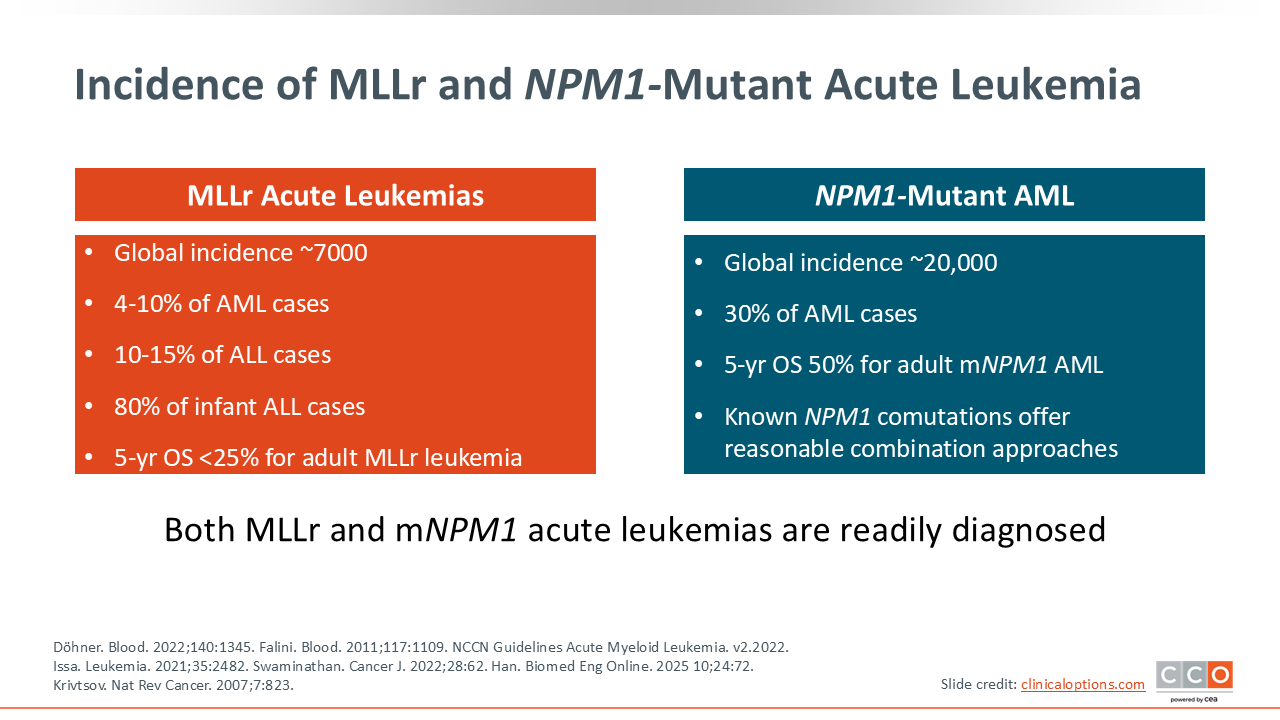
Menin inhibitors are a new class of therapies that target specific subtypes of acute leukemias. Specifically, patients with acute leukemias that have an MLL rearrangement, also known as a KMT2Ar, or with mNPM1 may benefit from menin inhibitors.
The global incidence of acute leukemias with KMT2Ar is approximately 7000 cases including approximately 4%-10% of patients with AML.1 KMT2Ar is predominant in patients with therapy-related AML or AML that is a direct result of cytotoxic chemotherapy or radiation received for a different malignancy.
De novo KMT2Ar ALL occurs in 10%-15% of cases with a special subtype of ALL in which up to 80% of infants have a KMT2Ar genotype.2 Adults with KMT2Ar disease typically have a very poor prognosis with a 5-year overall survival (OS) rate of less than 25%.3
These patients might go into remission with intensive induction chemotherapy but often have monocytic and extramedullary disease and rapidly relapse out of remission even after an allogeneic hematopoietic stem cell transplant (HSCT). It is difficult to induce a remission with standard therapy after this type of relapse.
NPM1-mutated AML is actually quite common. NPM1 is the most common mutation present in patients with newly diagnosed AML, representing 30% of cases with a global incidence of approximately 20,000.1,4
NPM1 mutations by themselves are characterized in the favorable risk category for patients with AML.5 The primary challenge is that NPM1 mutations frequently co-occur with additional mutations, which can reclassify affected cases from the favorable-risk category to the intermediate-risk category. One prevalent and specific example is co-occurrence with FLT3 mutations.6 Even when a patient has favorable-risk AML based on mNPM1 status, once the patient has relapsed, they are no longer characterized in the favorable risk category.
This is an important point to note. The risk stratification of patients with AML applies to patients with newly diagnosed disease.
All relapsed AML is considered unfavorable, and the patient's risk of not responding to standard therapies is very high. For these patients with R/R mNPM1-AML, it is important to develop novel therapies.7
Pathogenesis of KMT2A-Rearranged NPM1-Mutant Acute Leukemias and Menin Inhibitors
Eytan Stein, MD:
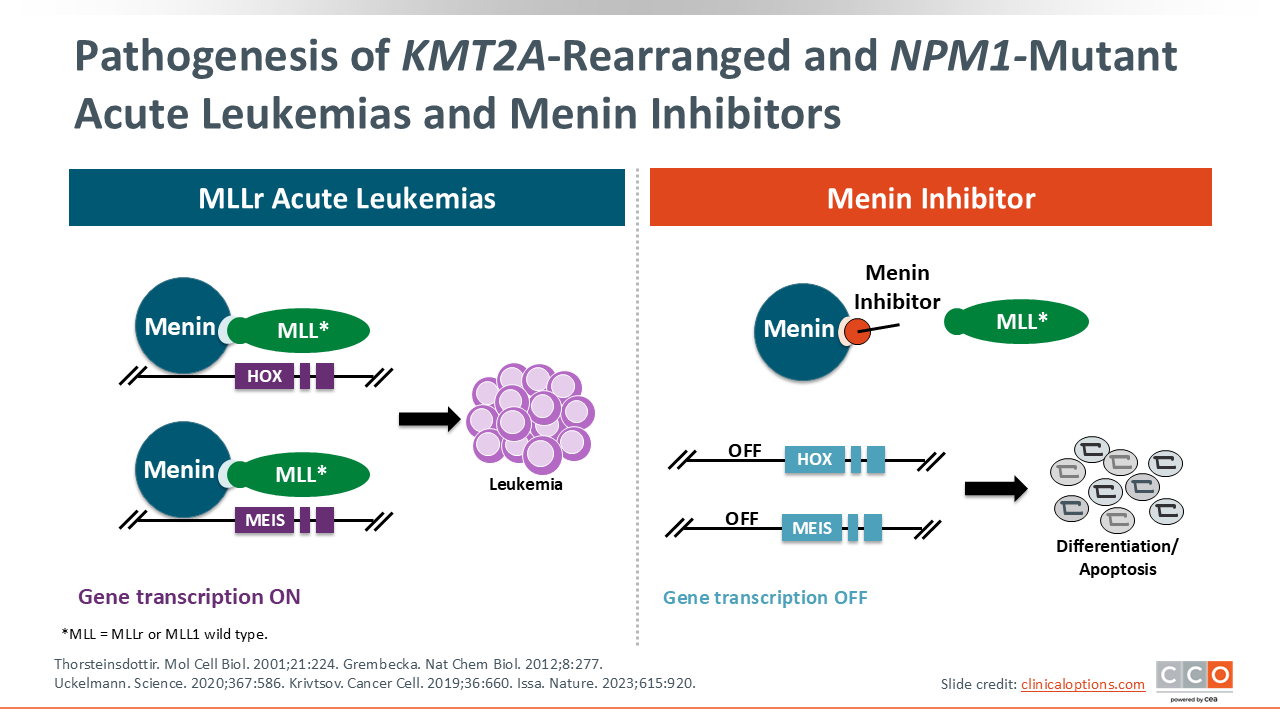
To understand why we use menin inhibitors, knowledge of menin’s mechanism to promote the development of acute leukemia is needed. Menin is an adapter protein that binds to MLL. MLL can exist in an abnormal form in KMT2Ar acute leukemias or in a normal form in mNPM1 acute leukemias. When menin binds to MLL—whether it is with KMT2Ar or with mNPM1—upregulation of HOX genes is promoted. This, in turn, promotes leukemogenesis.8
Due to this mechanism, an inhibitor which blocks the interaction between menin and MLL, turns off the upregulated HOX gene program. This allows leukemic blasts to differentiate and become normal, healthy cells.9-11 This mechanism was tested extensively in preclinical studies. Eventually, menin inhibitors were brought into clinical trials.12
AUGMENT-101: Revumenib Monotherapy in R/R KMT2Ar and mNPM1 Acute Leukemia
Eytan Stein, MD:
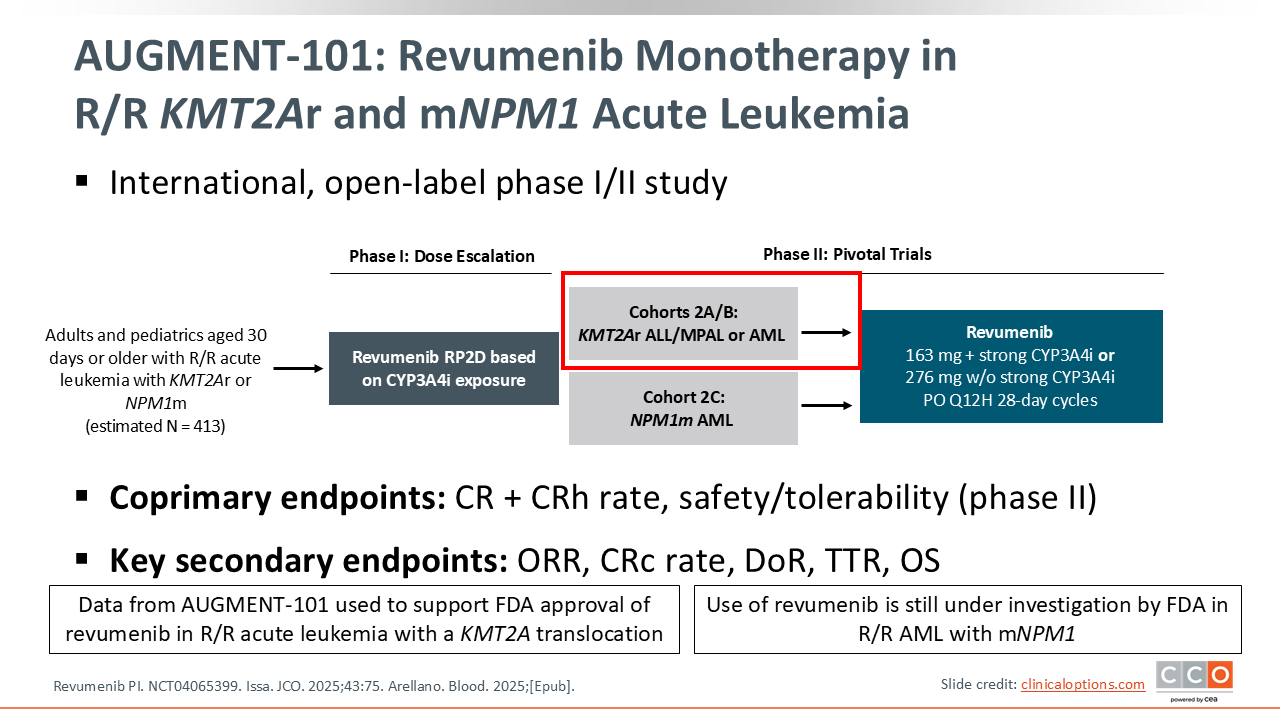
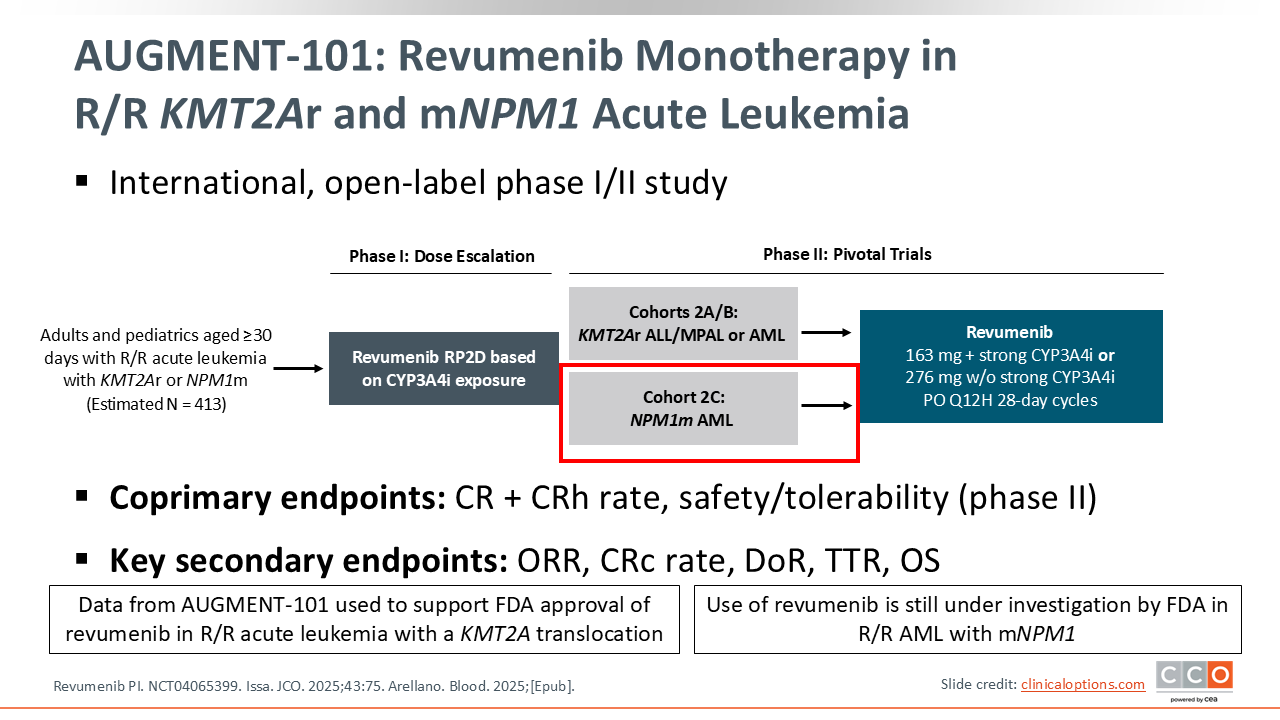
Revumenib is a novel menin inhibitor that was approved by the FDA in 2024 for the treatment of R/R acute leukemia with a KMT2A translocation in adult and pediatric patients 1 year of age or older.13
The original study that led to the approval of revumenib was the phase I/II AUGMENT-101 trial, which enrolled patients with R/R AML, ALL, or mixed phenotype acute leukemia with a KMT2Ar or mNPM1. This trial was somewhat unique in that it enrolled both adult and pediatric patients, including infants who were at least 30 days old. After the recommended phase II dose (RP2D) was determined, 2 subarms of the study were enrolled in a phase II component. One of the cohorts included patients with KMT2Ar. The other cohort was for patients with mNPM1.
The primary endpoints for the study were the rate of complete remission (CR) and complete remission with partial hematologic recovery (CRh) as well as safety and tolerability. Secondary endpoints included overall response rate (ORR), duration of response (DoR), and the time to response.
AUGMENT-101: Efficacy in R/R Acute Leukemia With KMT2Ar
Eytan Stein, MD:
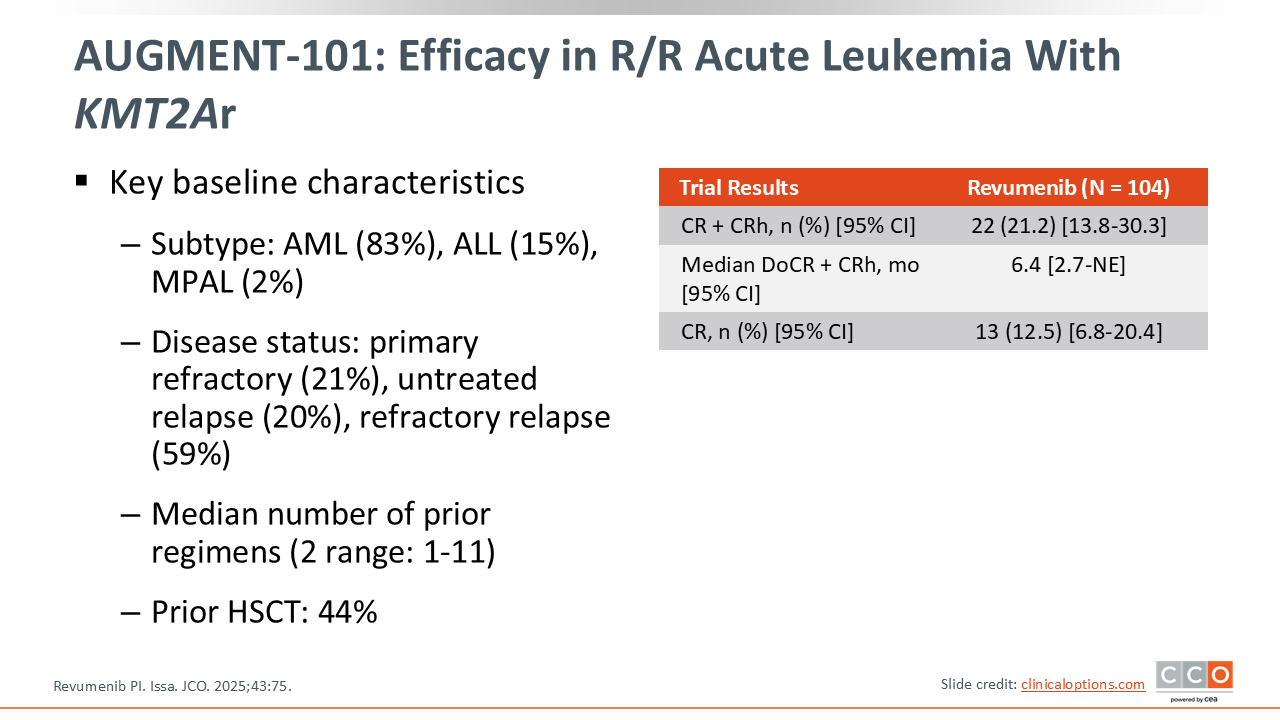
There are different types of KMT2Ar. The most common types of enrolled in this trial were patients with (9;11) translocations, (11;19) translocations, and (6;11) translocations. It is important to note that 44% of the patients in this trial had undergone a prior allogeneic HCT. This indicates that patients who have R/R acute leukemia with a KMT2Ar often have failed an allogeneic HCT, making them a particularly difficult group to treat. These patients typically don't respond to any of our conventional chemotherapy regimens. Revumenib treatment resulted in a combined CR plus CRh rate of 21.2% with a median response duration of 6.4 months.13 These results supported the approval of revumenib for patients with R/R acute leukemias and KMT2Ar and can make a significant difference in these patients' lives.
AUGMENT-101: Revumenib Monotherapy in R/R KMT2Ar and mNPM1 Acute Leukemia
Eytan Stein, MD:
Revumenib has now been submitted to the FDA for a supplemental new drug application pursuing an approval for patients with R/R mNPM1 AML.
In the R/R AML with mNPM1 cohort of the AUGMENT-101 trial, there were 84 patients evaluable for safety and 64 patients evaluable for efficacy, respectively. The discrepancy in sample sizes for this analysis was attributable to 20 patients having received at least 1 dose of the drug without having yet completed 6 months of study participation. As a result, these 20 patients were not included in the protocol-defined efficacy population (NCT04065399).14
Of interest, many of these patients have co-occurring mutations: 34% have co-occurring FLT3 internal tandem duplications (FLT3-ITD), 6% have co-occurring FLT3 tyrosine kinase domain mutations, and 13% have co-occurring IDH1 or IDH2 mutations, respectively. Each of these mutations can overlap with one another meaning there could be a patient who has an mNPM1, a FLT3 mutation, and an IDH mutation. More than 1 in 3 patients (35.9%) had received 3 or more prior lines of therapy with 75% having received prior venetoclax even though patients with mNPM1 AML tend to respond well to venetoclax. In addition, only 22% had received an allogeneic HCT because these patients are favorable risk mNPM1 AML who are either cured without an allogeneic HCT or are less likely to relapse after one.13,14
AUGMENT-101: Responses Were Rapid and Durable in R/R mNPM1 AML
Eytan Stein, MD:
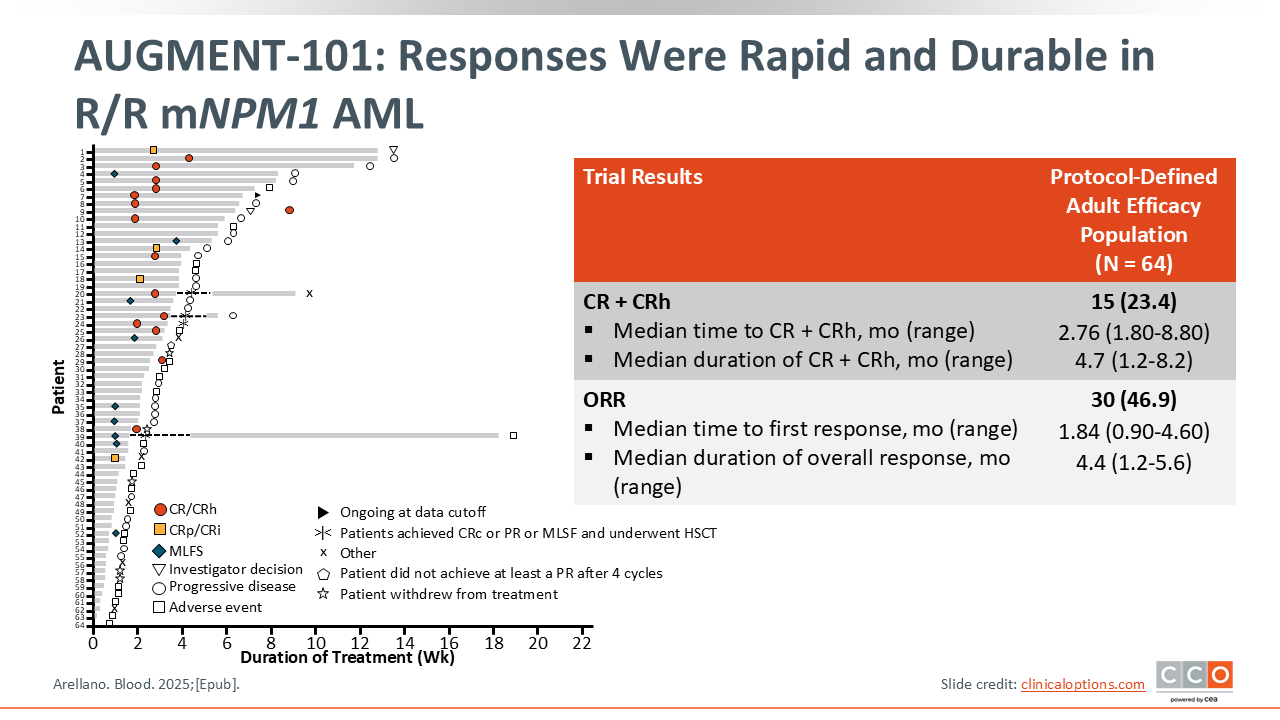
The rate of CR plus CRh for patients with R/R mNPM1 AML on revumenib is 23.4% for the protocol-defined adult efficacy population with the median duration of CR and CRh at 4.7 months.
The rate of measurable residual disease (MRD) negativity in patients who achieved a CR or CRh is actually quite high at 64%, suggesting the effect of a single-agent menin inhibitor in patients with R/R mNPM1 is not restricted to getting patients into remission, but rather extremely deep remissions. These deep remissions lack molecular or immunophenotypic evidence of persistent AML. As noted on the graph, there were a few patients who received revumenib, went into remission, received an allogeneic HCT and went back on maintenance revumenib after transplant.
The responses in patients with mNPM1 AML seemed to be profound and consistent across patient subgroups analyzed by age, sex, number of prior lines of therapy, prior allogeneic HCT, prior venetoclax, and IDH1 or FLT3 mutation status.14
AUGMENT-101: Safety Results From Phase II R/R mNPM1 AML Cohort
Eytan Stein, MD:
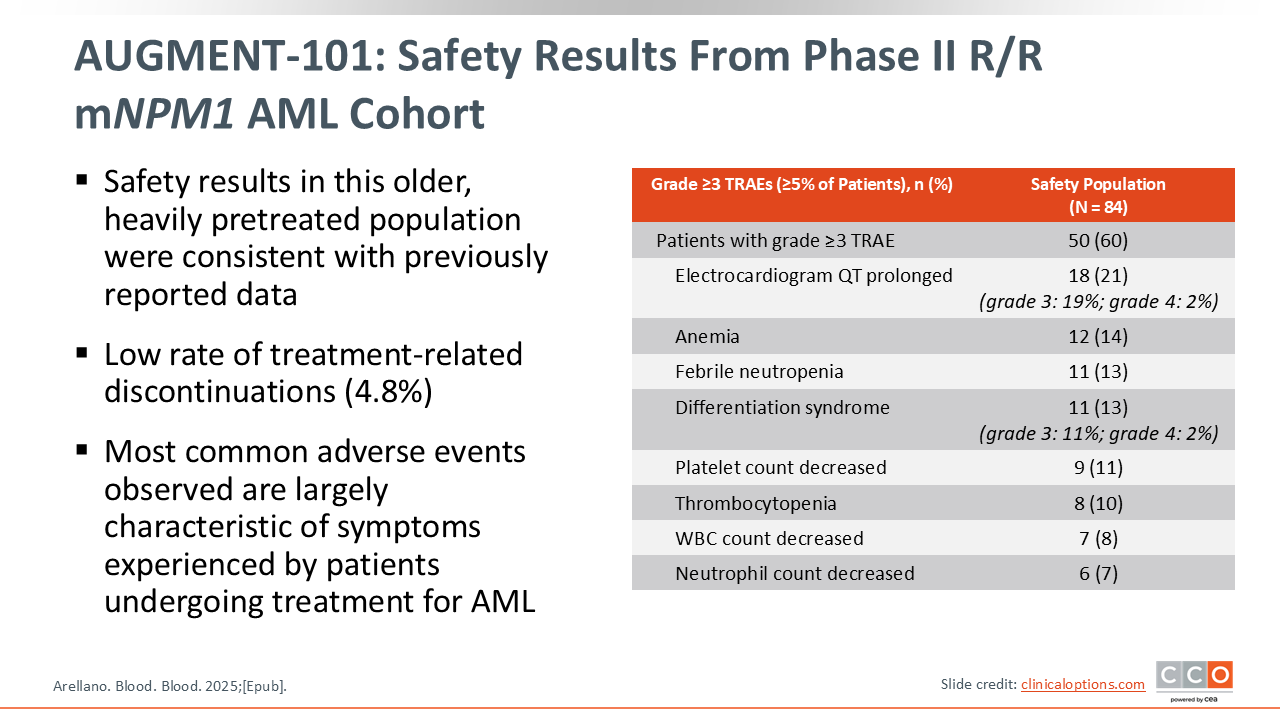
There are a few key points to be aware of regarding the safety of revumenib for patients with KMT2Ar and/or mNPM1 AML. First, revumenib can cause QT prolongation. The rate of grade 3 QT prolongation was 19% and 2% of patients experienced grade 4 QT prolongation.14 Second, there is a risk of DS with grade 3 events reported in 11% of patients and grade 4 events in 2% of patients. DS is reported across all menin inhibitors and necessitates very careful surveillance. If you think a patient is experiencing DS, you need to give that patient steroids, typically dexamethasone 10 mg twice a day, because DS can become very serious.14
Beat AML Trial: Revumenib + VEN/AZA in Newly Diagnosed AML With NPM1m or KMT2Ar
Eytan Stein, MD:
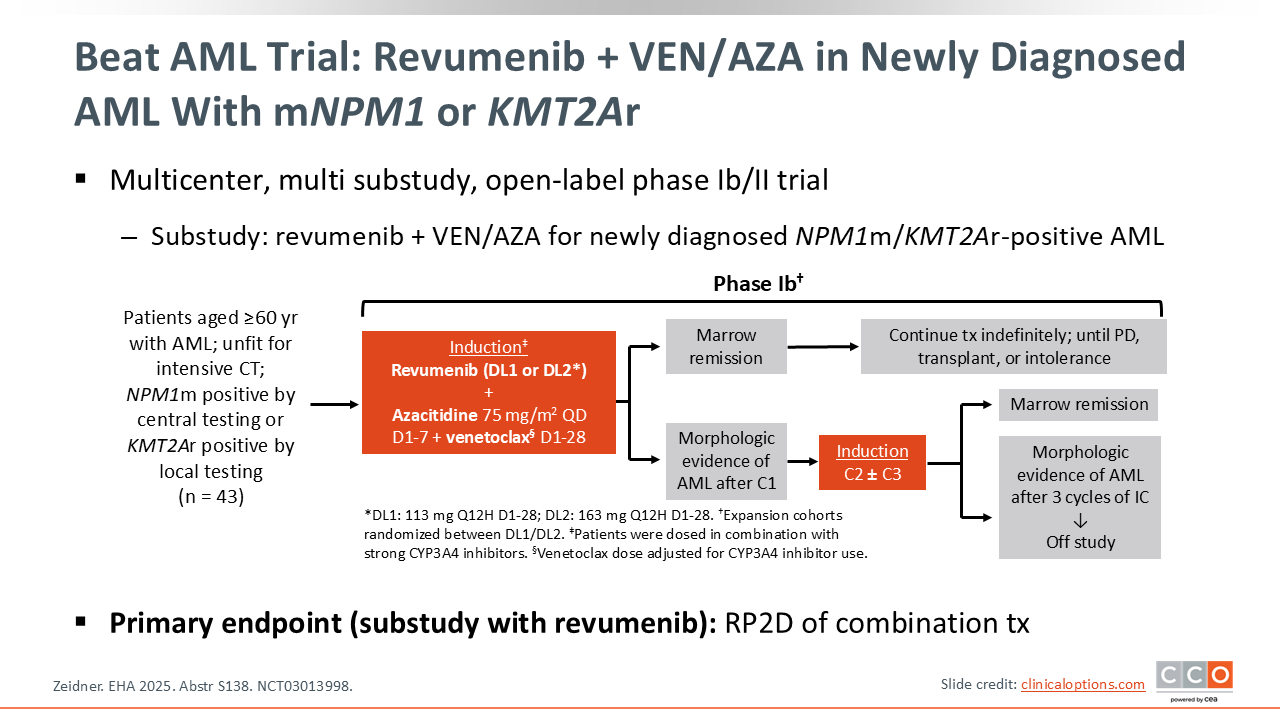
There also are data supporting the frontline use of revumenib in older, newly diagnosed adults with either mNPM1 or KMT2Ar AML. In the BEAT AML trial, patients received a triplet regimen of azacitidine plus venetoclax plus revumenib in the frontline setting.15,16
This phase Ib/II study enrolled patients into 2 revumenib dose cohorts in combination with standard dosing for azacitidine and venetoclax. Patients who achieved a remission continued the triplet therapy until progression, transplant, or intolerance. Patients who did not achieve a CR after 3 cycles of therapy were taken off study for futility.
Out of all 43 patients on trial, the median age was 70 years with 39.5% being older than 75 years; 21.4% of patients had co-occurring NRAS mutations, 11.9% had co-occurring KRAS mutations, and 25.6% had FLT3-ITD mutations.16
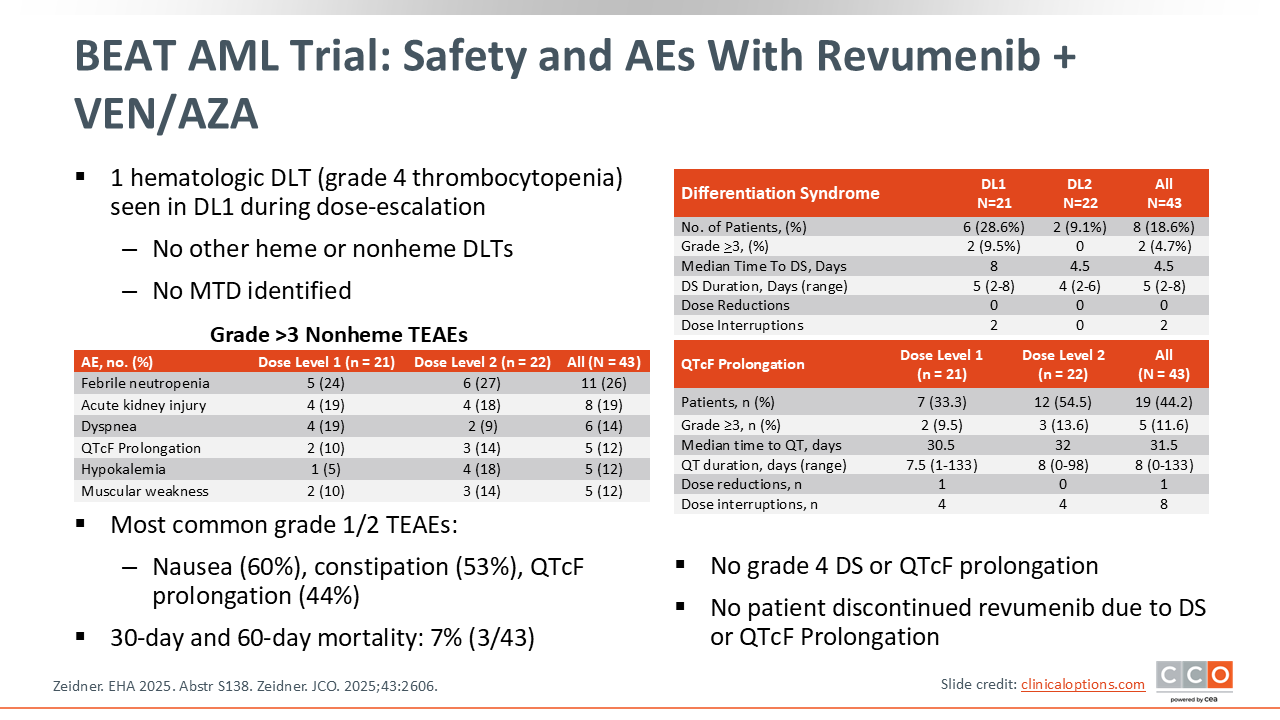
BEAT AML Trial: Safety and AEs of Revumenib + VEN/AZA
Eytan Stein, MD:
There was 1 hematologic dose-limiting toxicity observed at dose level 1 (113 mg) of the dose escalation. There were no other dose-limiting toxicities, and no maximum tolerated dose was identified. The most common grade 1/2 treatment-emergent adverse events (TEAEs) were nausea, constipation, and QT prolongation.15,16
The 30-day and 60-day mortality was 7%, although, if you look beyond 60 days, there were patients who died while on therapy. To my knowledge, the reasons for those deaths have not been fully identified. There were no grade 4 DS or grade 4 QTc prolongation events reported.15,16
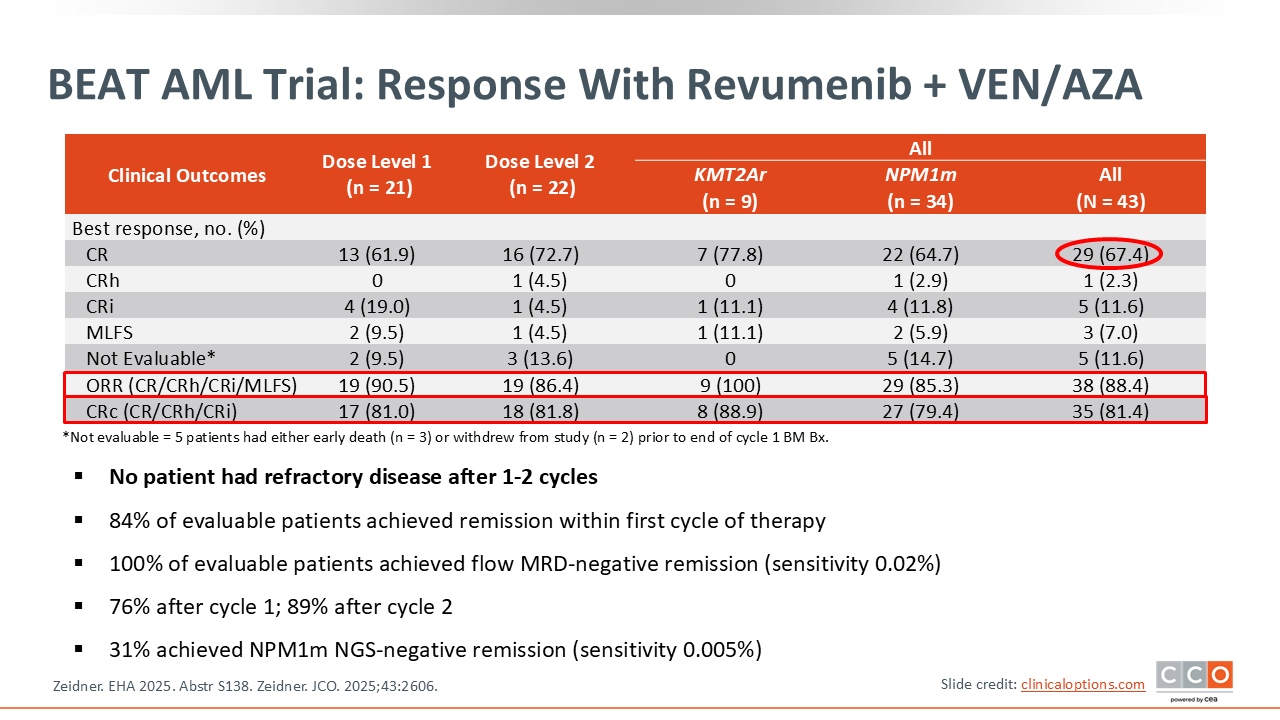
BEAT AML Trial: Response With Revumenib + VEN/AZA
Eytan Stein, MD:
Across all patients, the CR rate is 67.4% and the ORR is 88.4% which is quite high. Patients with mNPM1 AML (n = 34) had an ORR of 85.3% while the patients with KMT2Ar disease (n = 9) had an ORR of 100%.15,16
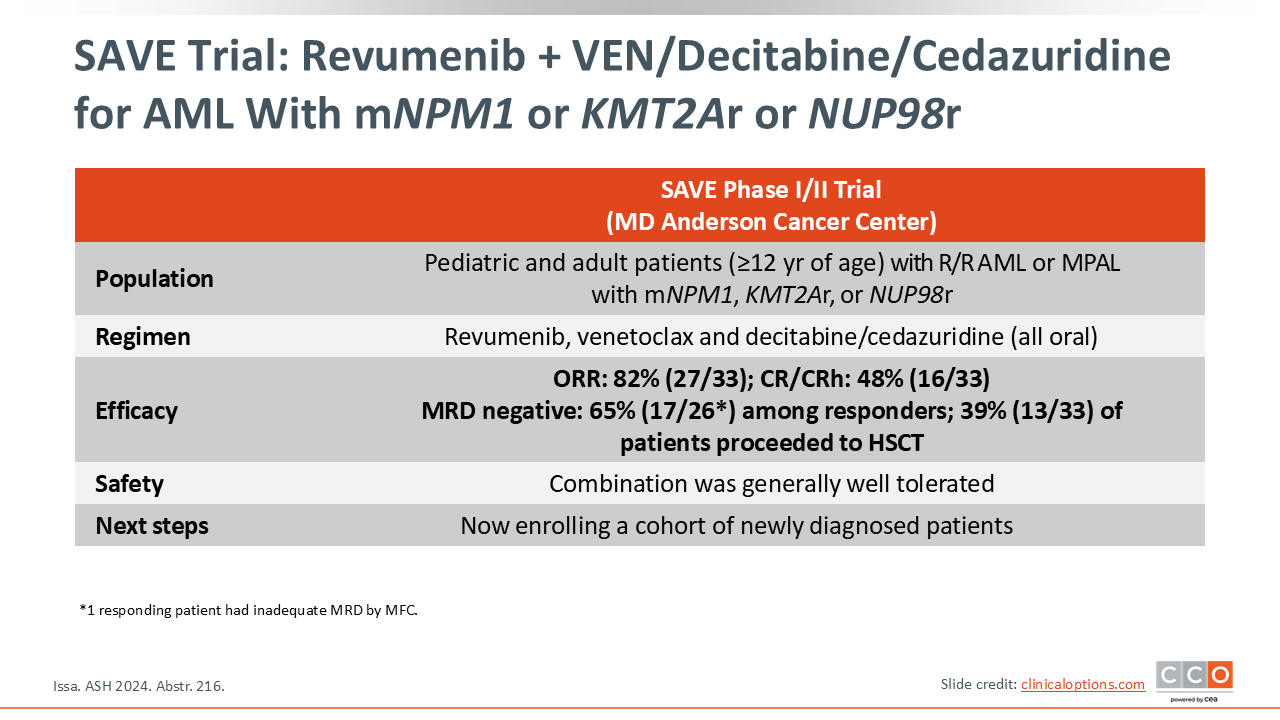
SAVE Clinical Trial
Eytan Stein, MD:
The phase I/II SAVE trial at the MD Anderson Cancer Center is evaluating an all-oral triplet combination with the hypomethylating agent decitabine/cedazuridine plus venetoclax plus revumenib in R/R AML. The reported ORR was 82% with a combined CR and CRh of 48%; 65% of the patients were MRD negative and 39 proceeded to an allogeneic HCT. This trial is now enrolling a cohort of patients with newly diagnosed disease.17
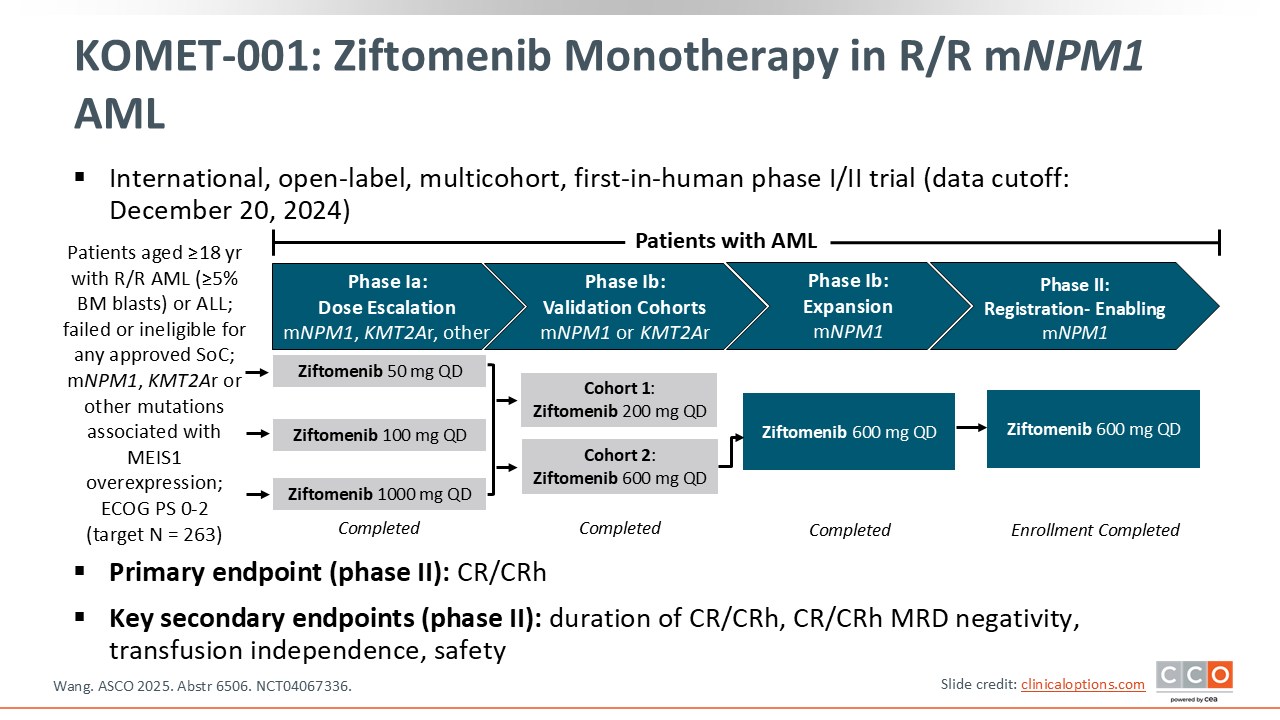
KOMET-001: Ziftomenib Monotherapy in R/R mNPM1 AML
Eunice Wang, MD:
Now we will discuss ziftomenib, a second menin inhibitor that is currently under review by the FDA for potential approval later in 2025.
The main study with this drug is the first-in-human KOMET-001 phase I/II trial which is evaluating ziftomenib in patients with R/R AML. This trial includes multiple substudies (NCT04067336). The initial dose-escalation phase of KOMET-001 examined the safety and tolerability of ziftomenib in the dose range of 50 mg to 1000 mg daily. The phase Ib stage included 2 validation cohorts of monotherapy in adult patients with mNPM1 and KMT2Ar R/R AML. The phase II cohort examined the use of ziftomenib at 600 mg daily specifically in patients with mNPM1 R/R AML. Results of this potentially registration-enabling cohort were recently presented at the ASCO 2025 meeting.18
The primary endpoint of the initial cohorts was safety and tolerability. The early cohorts established 600 mg as the recommended target dose for further evaluation. Like other menin inhibitor studies, on-target DS was recognized as a potentially life-threatening complication. This led the investigators to halt monotherapy development in patients with KMT2Ar disease and proceed with ziftomenib therapy in patients who had mNPM1 R/R AML only. Approximately one third of patients with newly diagnosed AML harbor mutations in the NPM1 gene, and approximately half of these patients will experience relapses that will require salvage regimens. A pooled analysis of the phase Ib/II stages included 112 patients with a median age of 69 years (range: 22-86). These patients were heavily pretreated and had received a median of 2 lines of prior therapy (range: 1-7). Approximately one quarter of patients had prior allogeneic HCT, 60% had prior venetoclax therapy, and 53% had a concomitant FLT3 mutation, either ITD or TKD.18
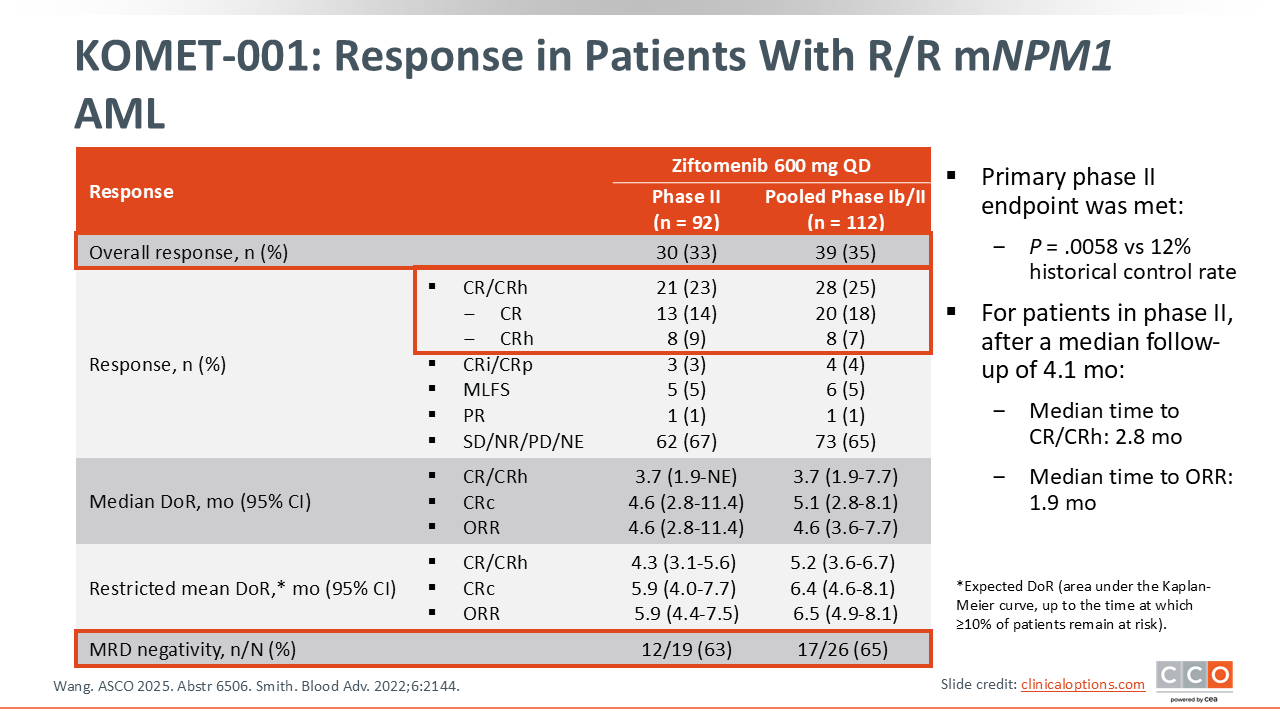
KOMET-001: R/R mNPM1 AML Response
Eunice Wang, MD:
The results of the pooled phase Ib and II cohorts demonstrated convincing clinical efficacy of ziftomenib in patients with R/R mNPM1 AML. In these heavily pretreated patients, the CR plus CRh (CRc) rate was 25%, with 18% CR and 7% CRh. The median DoR was 5.1 months for patients who achieved CRc. In addition, 65% of ziftomenib-treated patients achieving CRc were determined to be MRD negative using a centrally tested molecular screening for mNPM1 disease.
Patients with FLT3 or IDH1 and IDH2 comutations had ORRs similar to the overall patient population. Moreover, patients who had prior HSCT or prior venetoclax also had response rates similar to the overall patient population. These data differ from revumenib studies where prior venetoclax therapy appeared to confer resistance to this specific menin inhibitor therapy.
Of note, this phase II cohort was designed with the primary endpoint of CR/CRh. The historical control CR/CRh used for this study to predict the expected response rate of salvage chemotherapy in this patient population was 12%.19 The CR plus CRh rate of 25% in the overall population, as well as 23% in the phase II cohort, was statistically superior to this historical control rate with a P value of .0058.18
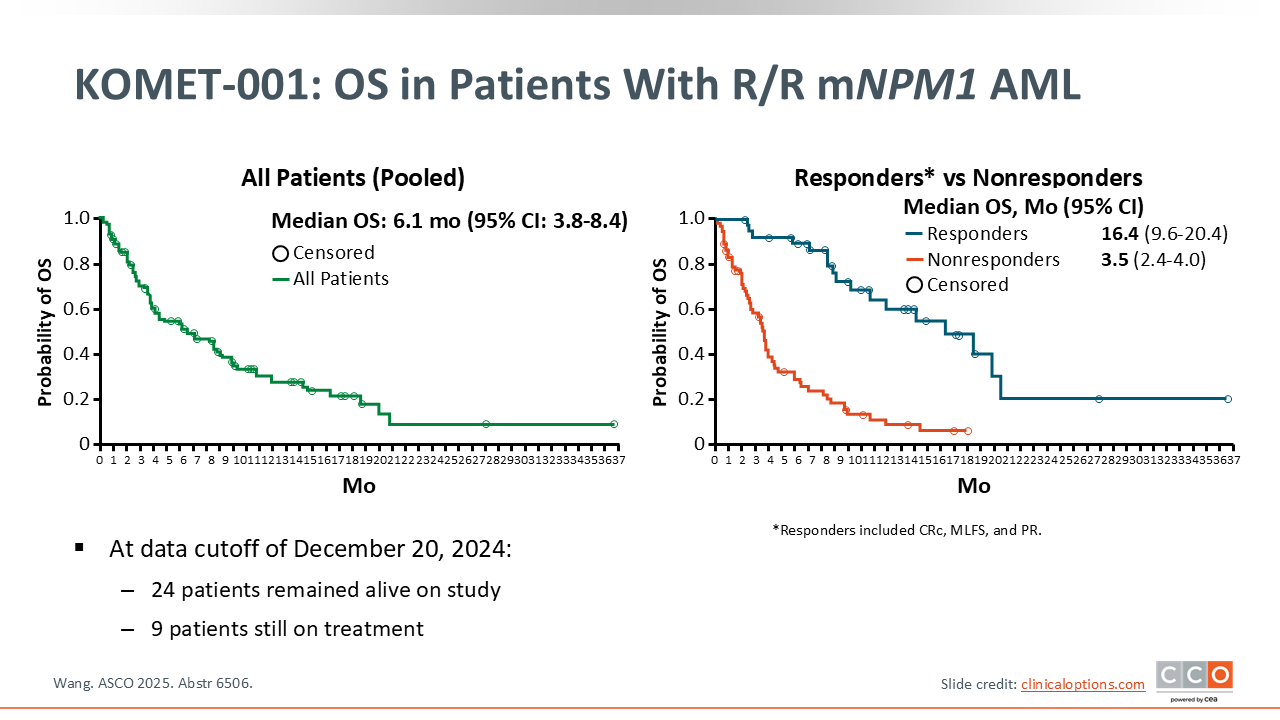
KOMET-001: OS in Patients With R/R mNPM1 AML
Eunice Wang, MD:
Censoring for transplant, the median OS was 6.1 months. Although we know that responders always do better than nonresponders, the median OS of the ziftomenib responders was an impressive 16.4 months as opposed to a median OS of 3.5 months in the nonresponding patient population, consistent with historical expectations. At the time of data cutoff, 24 patients remained alive on study, and 9 of 92 patients in the phase II cohort were still on treatment.18
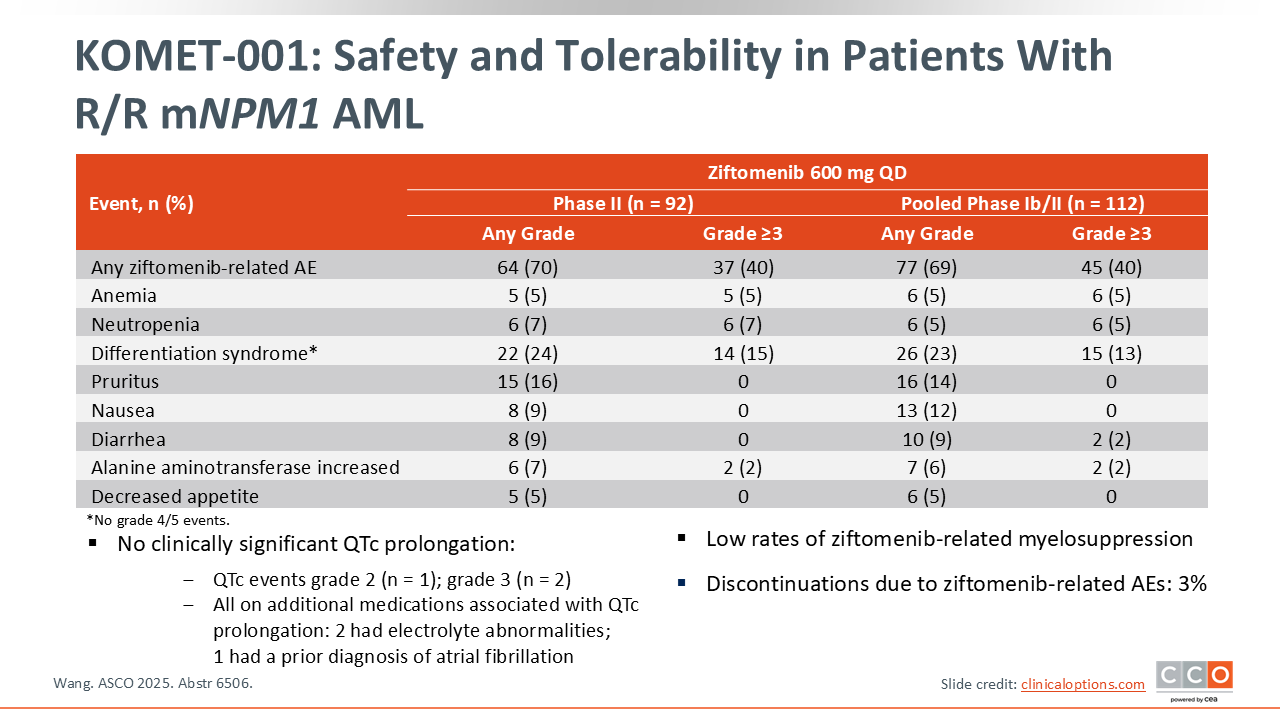
Safety and Tolerability in Patients With R/R mNPM1 AML
Eunice Wang, MD:
There are some distinctions to be made between the adverse events (AEs) experienced with ziftomenib vs revumenib. Approximately two thirds of patients experienced a ziftomenib-related AE, but there was no evidence of clinically significant QTc prolongation in this trial. Although 3 patients experienced QTc prolongation on study, all had other factors that may have contributed to QTc prolongation, including other medications, electrolyte abnormalities, and a previous diagnosis of atrial fibrillation.
Grade ≥3 anemia and neutropenia were reported in approximately 5% of patients. Although DS was reported in 24% of patients, only 13% had grade 3 events, and there were no grade 4 or 5 events. Treatment-related AEs associated with ziftomenib led to discontinuation in 3% of patients. Overall, this drug as a monotherapy appeared to be very well-tolerated.18
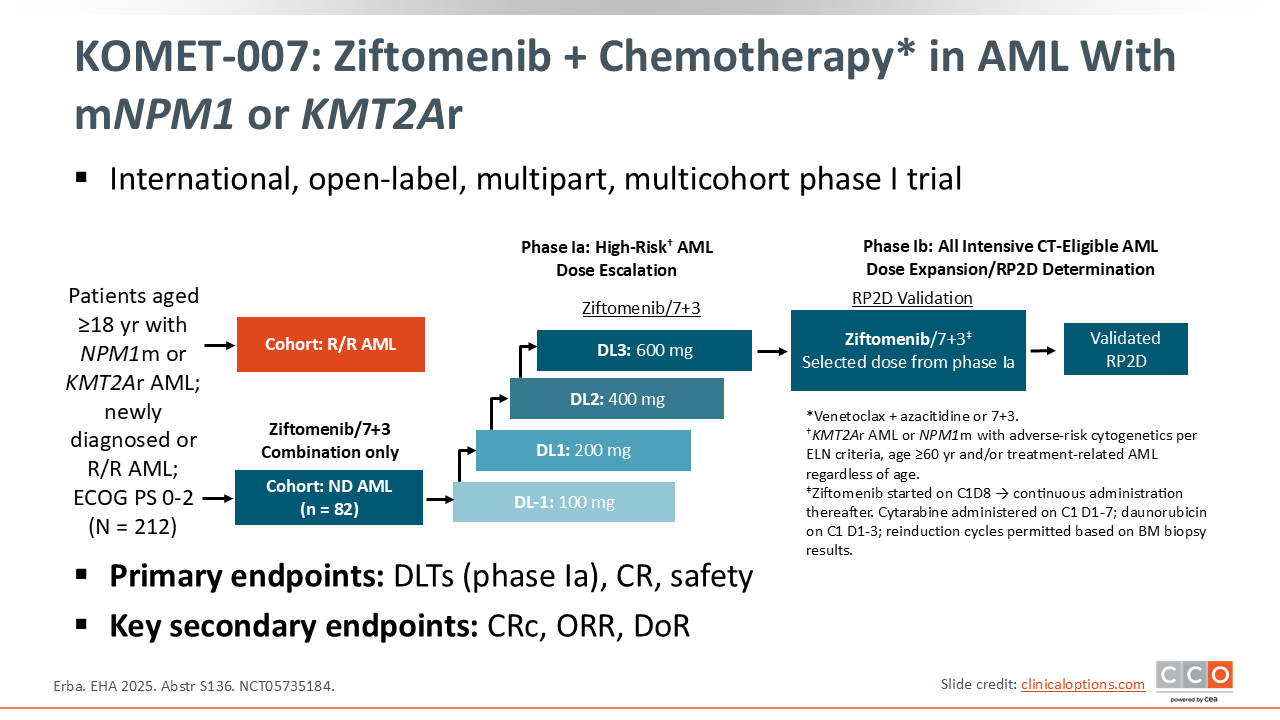
KOMET-007: Ziftomenib + Chemotherapy in AML
Eunice Wang, MD:
KOMET-007, an international open-label, multipart, multicohort phase I study evaluating ziftomenib in combination with chemotherapy for patients with R/R or newly diagnosed AML characterized by KMT2Ar or mNPM1 has been reported in recent EHA (2025) and ASH (2024) meetings. Subjects were enrolled in different treatment cohorts combining ziftomenib either with intensive (7+3) chemotherapy or less intensive (venetoclax plus azacitidine) chemotherapy based on the overall fitness and performance status of the patient. The target ziftomenib dose from the escalation portion was 600 mg which was also the RP2D. The primary endpoints were dose-limiting toxicity only for the phase Ia portion of the trial and CR and safety outcomes for phase Ib (NCT05735184).20
The average age of patients enrolled on this trial was 56 years, with patients with KMT2Ar AML having a lower median age of 43 years than those with mNPM1 at 60 years. Approximately 12% of patients had therapy-related AML, which is more common in patients with KMT2Ar. Approximately one third of patients had comutations in FLT3 or IDH1/IDH2.20
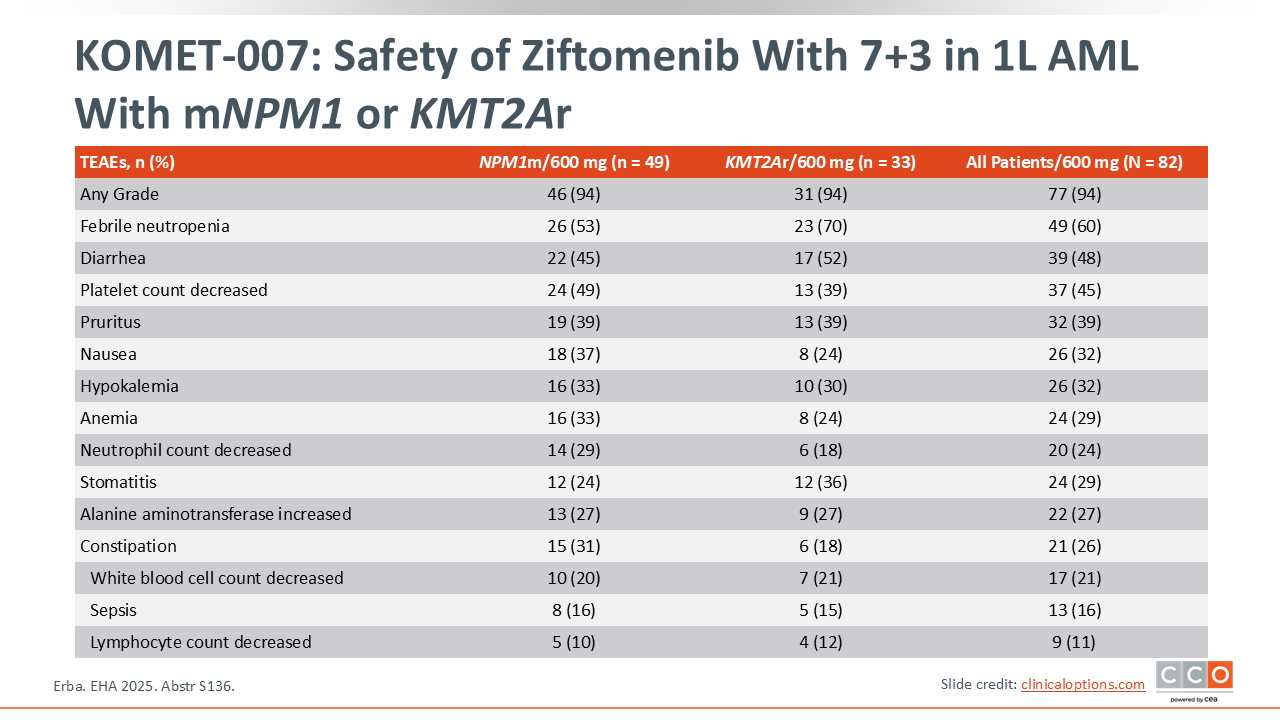
KOMET-007: Safety of Ziftomenib With 7+3 in 1L AML With mNPM1 or KMT2Ar
Eunice Wang, MD:
Early results demonstrate that ziftomenib did not significantly add to the overall toxicity of intensive chemotherapy with the 7+3 regimen. As expected, there were high rates of febrile neutropenia, as well as nausea, vomiting, thrombocytopenia, and anemia. A total of 82 patients developed DS with only 1 case that was grade 3, which was successfully mitigated. Two cases of QTc prolongation in patients on concomitant QTc prolongation medications were reported. Overall rates of sepsis and infection were low as expected.20
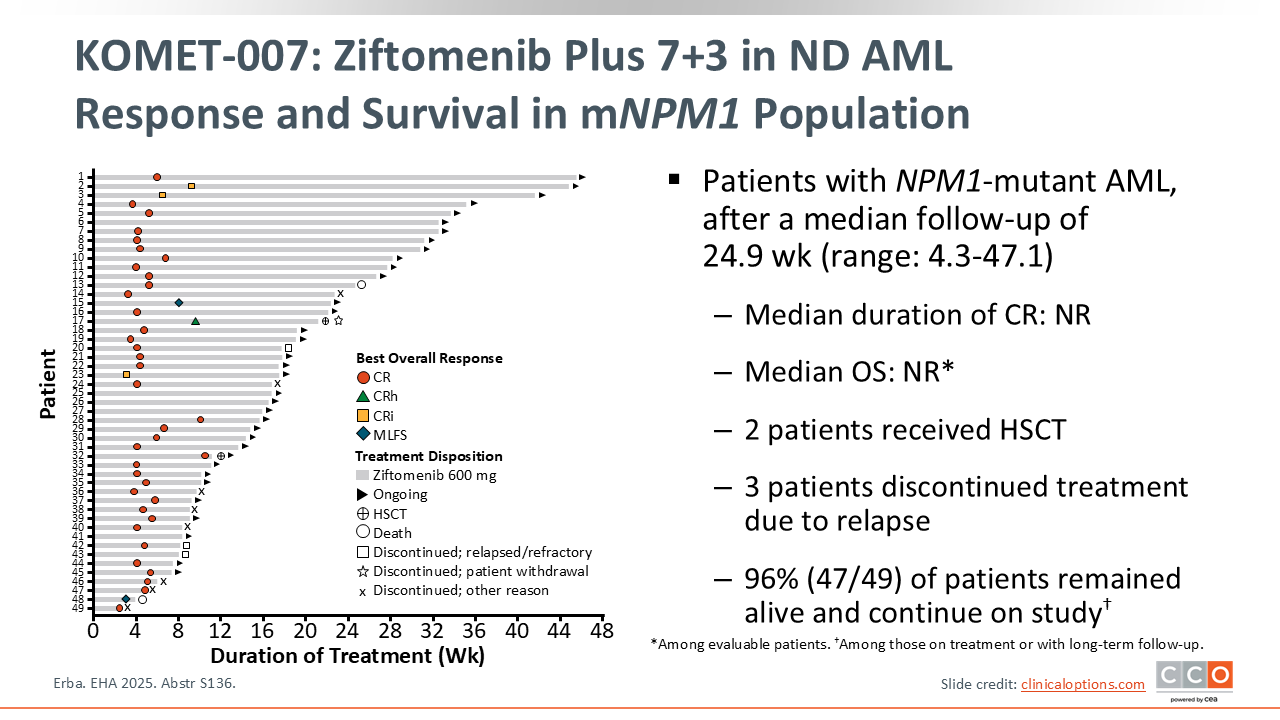
KOMET-007: Ziftomenib Plus 7+3 in ND AML Response and Survival in mNPM1 Population
Eunice Wang, MD:
The clinical activity of the ziftomenib/7+3 combination was highly promising. Among 71 evaluable patients, 92% achieved a CRc with a CR rate of 80%. The ORR was 94%. MRD negativity by central testing was achieved by 76% of all evaluable patients with a median time to achieving an MRD-negative CR of only 4.5 weeks.
Among patients with mNPM1 disease, 96% were still alive and continuing on study after a median follow-up of 24.9 weeks. The median duration of CR and the OS after 24 weeks was not reached. There have been 2 patients who received transplant and 3 patients who discontinued treatment due to relapse.20
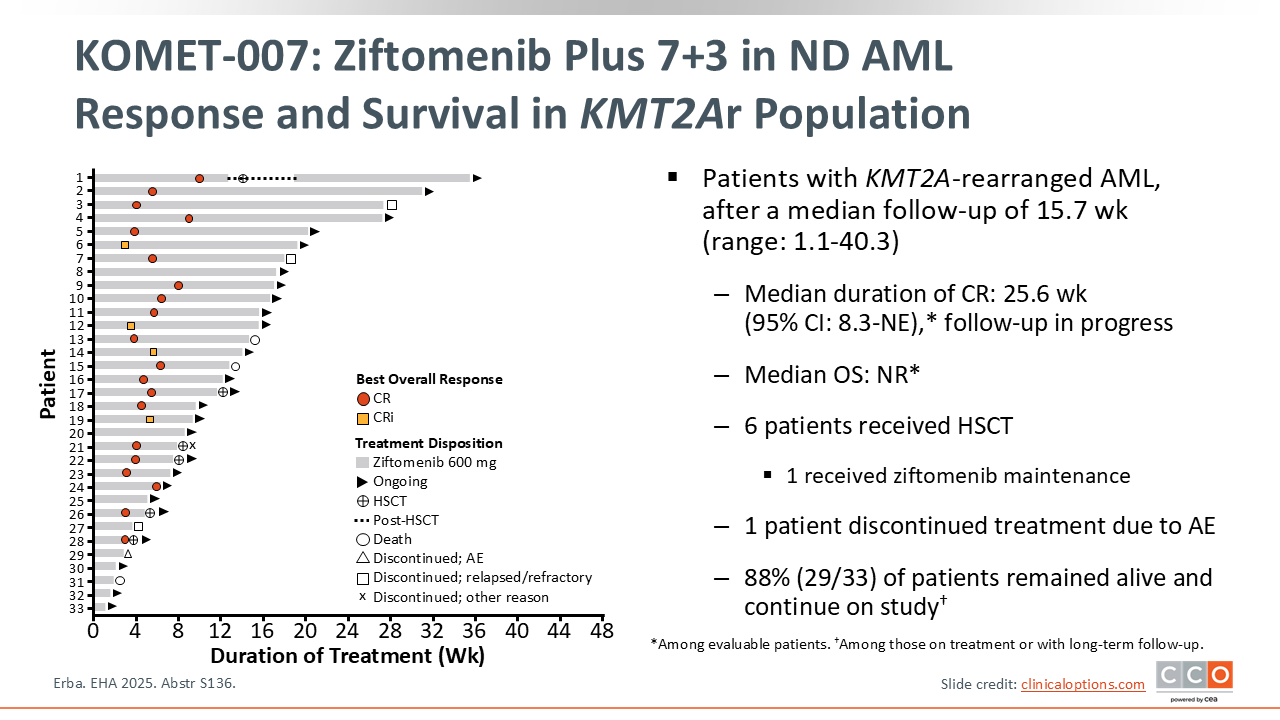
KOMET-007: Ziftomenib Plus 7+3 in ND AML Response and Survival in KMT2Ar Population
Eunice Wang, MD:
In the newly diagnosed KMT2Ar AML population treated with ziftomenib added to 7+3, with a median follow-up of 16 weeks, the median duration of CR was approximately 25 weeks, and the median OS has not been reached. Six patients have undergone subsequent allogeneic HSCT, with 1 receiving ziftomenib maintenance after transplant. Most patients with newly diagnosed KMT2Ar (88%) AML remain alive and on study.
Although KMT2Ar leukemias exposed to prior therapy may have underlying factors that predispose them to cytopenias, there was no evidence of prolonged count recovery or time to count recovery in these patients. Absolute neutrophil count (ANC) and platelet recovery occurred within 29-32 days.20
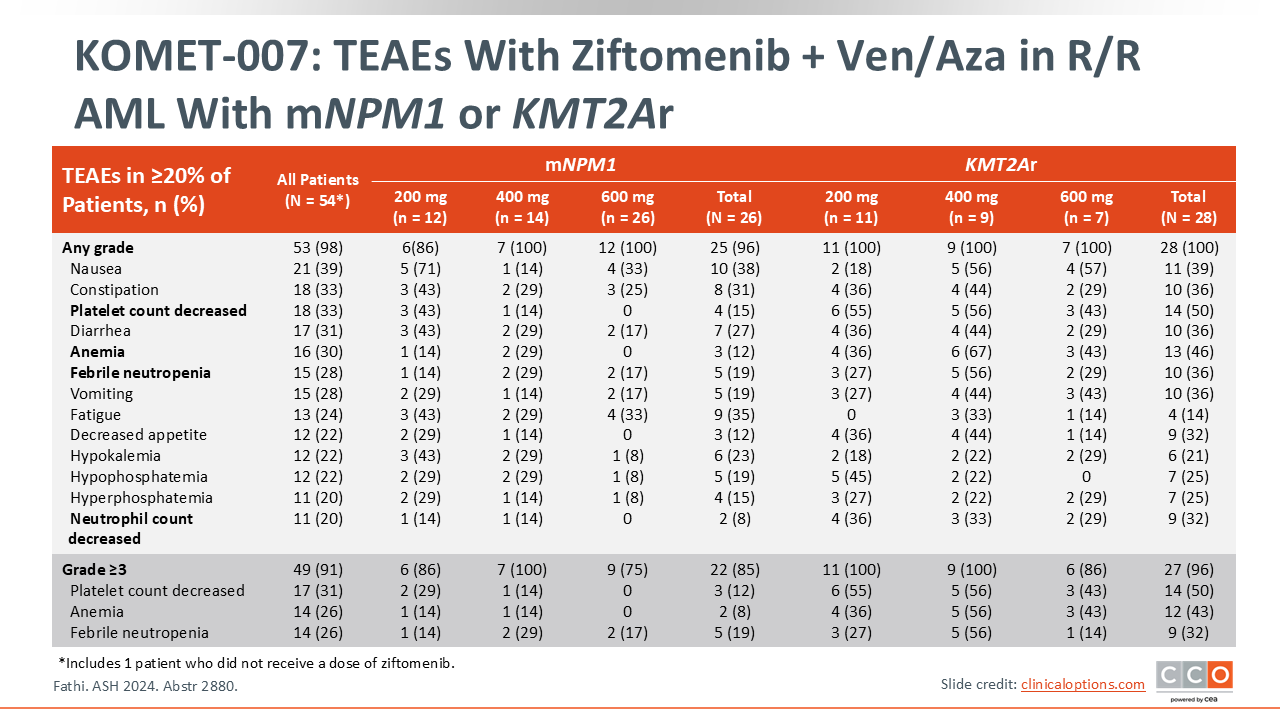
KOMET-007: TEAEs Occurring in ≥20% of R/R Patients
Eunice Wang, MD:
Now we will look at the separate dose escalation cohort of patients (n = 54) with R/R AML and mNPM1 or KMT2Ar who were treated with ziftomenib plus venetoclax/azacitidine in the KOMET-007 trial. In this analysis with a limited number of patients, select TEAE rates appeared to vary based on the presence of mNPM1 or KMT2Ar. Patients with mNPM1 and KMT2Ar had 15% and 50% decreased platelet counts (any grade), 19% and 36% febrile neutropenia (any grade), and 12% and 46% anemia (any grade) respectively, which is expected with this particular venetoclax/azacitidine backbone in R/R disease.21
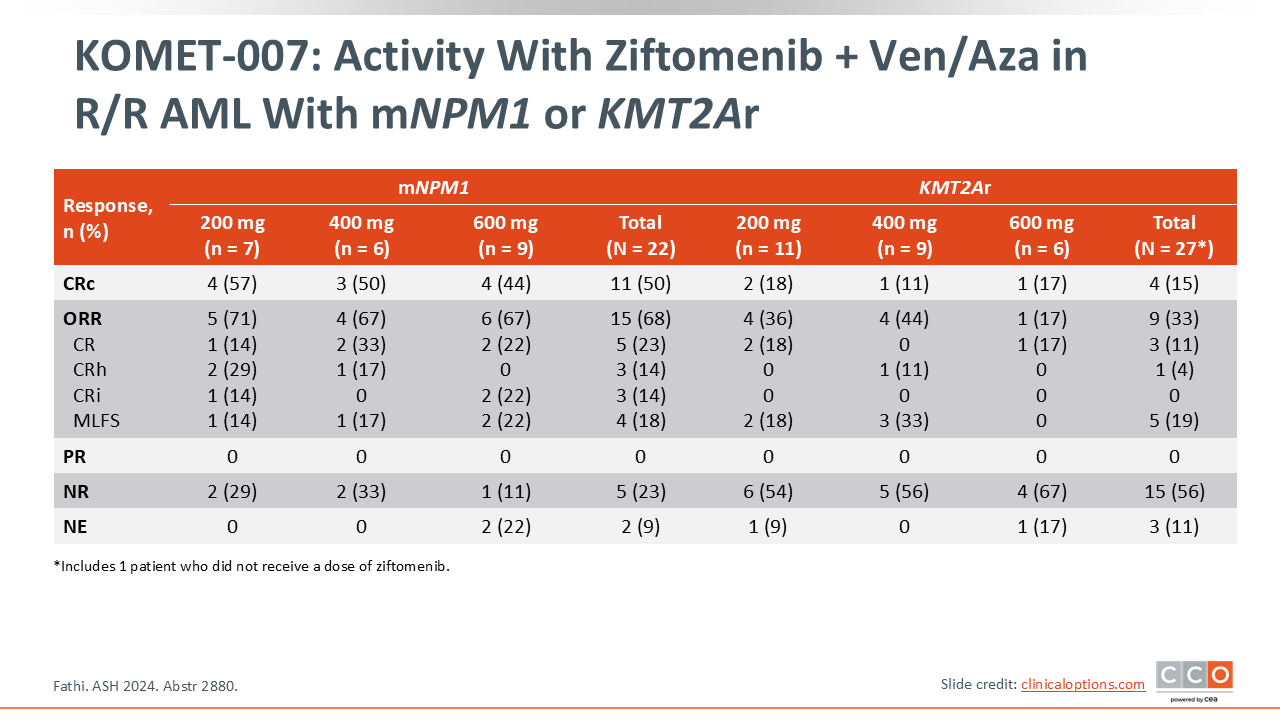
KOMET-007: Activity With Ziftomenib + Ven/Aza in R/R AML With mNPM1 or KMT2Ar
Eunice Wang, MD:
Half of patients in the KOMET-007 trial with R/R mNPM1 AML who received ziftomenib achieved a CRc, which was a considerable improvement from the CRc of 25% reported with ziftomenib monotherapy. Treatment with a venetoclax/azacitidine backbone alone would be expected to produce a CRc rate of approximately 20% or 30%. The CR rate in this patient population was 23% with an ORR of 68%.21
Among patients with R/R mNPM1 AML who were not previously exposed to venetoclax (n = 8), the CRc rate was 75% with a 100% ORR. In comparison, for patients with R/R mNPM1 AML and previous venetoclax exposure (n = 14), the CRc rate was 36% and the ORR was 50%. Also, among 11 patients (3 mNPM1, and 8 KMT2Ar) who had prior menin-inhibitor experience, 2 patients with KMT2Ar disease experienced a response to ziftomenib at 200 mg and 400 mg dose levels.21
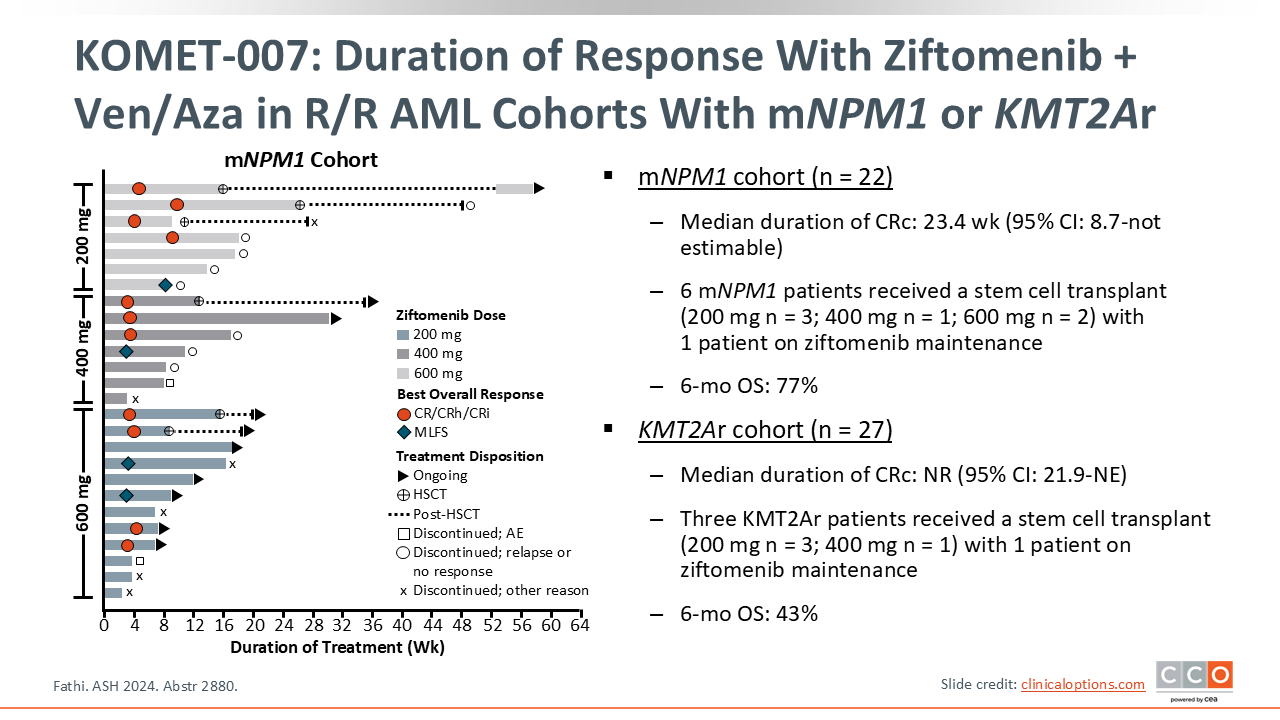
KOMET-007: Duration of Response With Ziftomenib + Ven/Aza in R/R AML Cohorts With mNPM1 or KMT2Ar
Eunice Wang, MD:
Six patients with R/R AML and mNPM1 who received ziftomenib plus venetoclax/azacitidine therapy received subsequent allogeneic HCT with 1 patient on ziftomenib maintenance therapy. The 6-month OS was 77% for these patients.
For patients with KMT2Ar AML, 3 patients received subsequent allogeneic HCT with 1 patient on ziftomenib maintenance therapy. The 6-month OS was 43% for these patients.
Patients with CRc recovered ANC and platelet counts as would be expected with the treatment backbone that was used. The ANC returned to ≥0.5x109/L and platelets returned to ≥50x109/L after 35 and 14 days, respectively after the first cycle of ziftomenib 600 mg.21
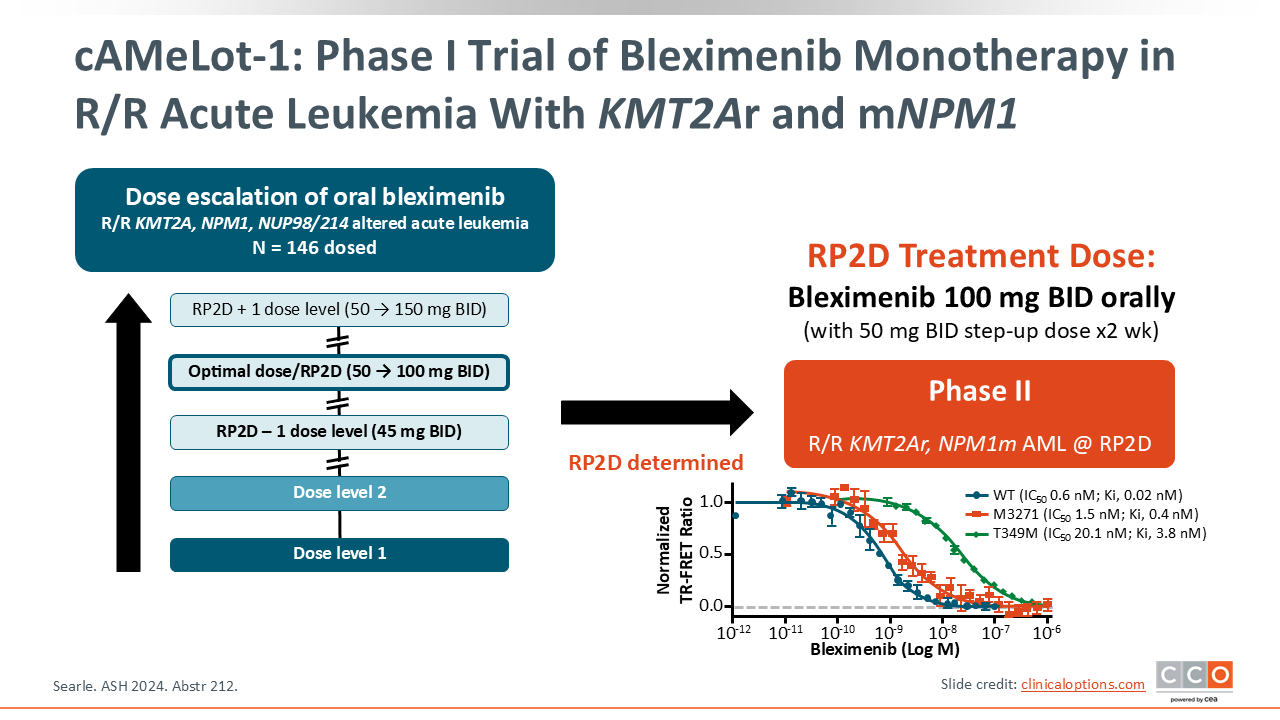
cAMeLot-1: Phase I Trial of Bleximenib Monotherapy in R/R Acute Leukemia With KMT2Ar and mNPM1
Eunice Wang, MD:
One of the most widely used menin inhibitors outside of the US is bleximenib. Bleximenib has shown clinical efficacy in patients with KMT2Ar and mNPM1 AML and is a new-generation agent that has demonstrated promising activity in leukemia cells with known inhibitor–resistant mutations in preclinical studies. Clinically, bleximenib is administered twice daily and has been evaluated at different doses ranging from 45 mg to 150 mg.22
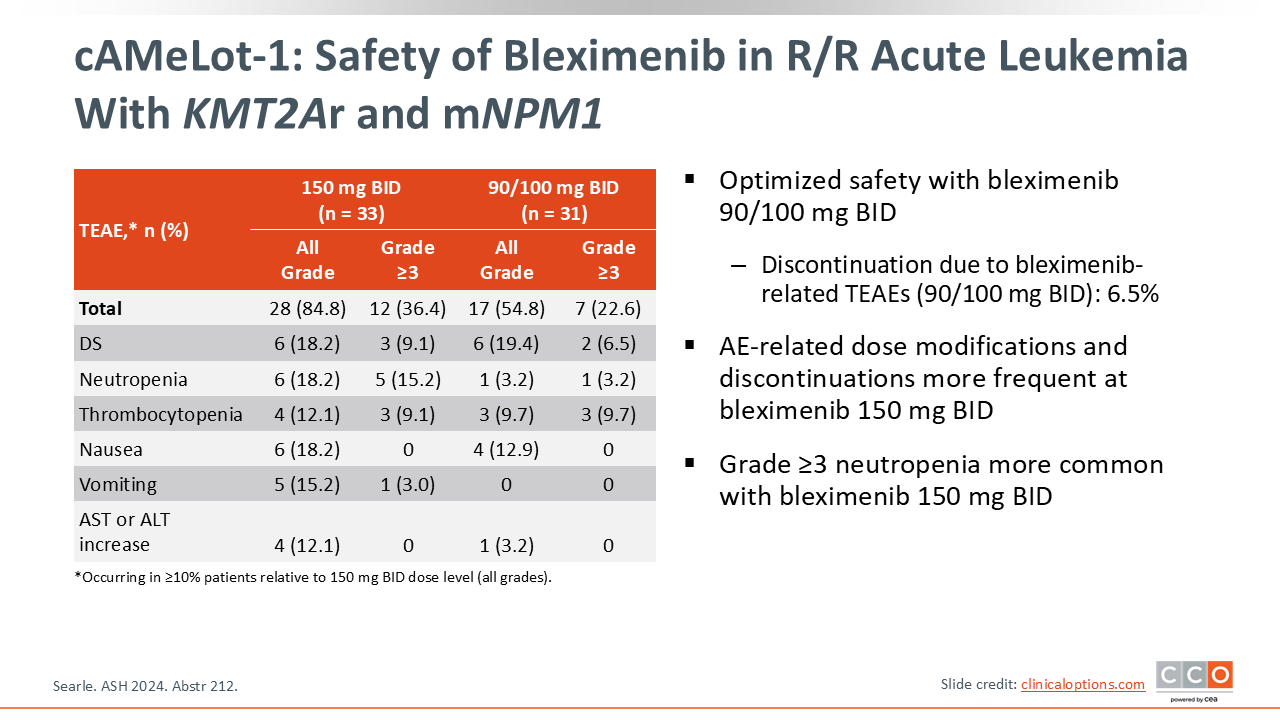
cAMeLot-1: Safety of Bleximenib in R/R Acute Leukemia With KMT2Ar and mNPM1
Eunice Wang, MD:
Bleximenib resulted in clinical DS in approximately 20% of the patient population. This is similar to what was reported with ziftomenib in the KOMET-001 trial at 24% and in the revumenib phase II trials.18,22 Approximately 6% to 9% of patients experienced grade ≥3 DS with bleximenib, similar to the results (13% DS) of revumenib in the mNPM1 AML patient cohort in AUGMENT trial.14
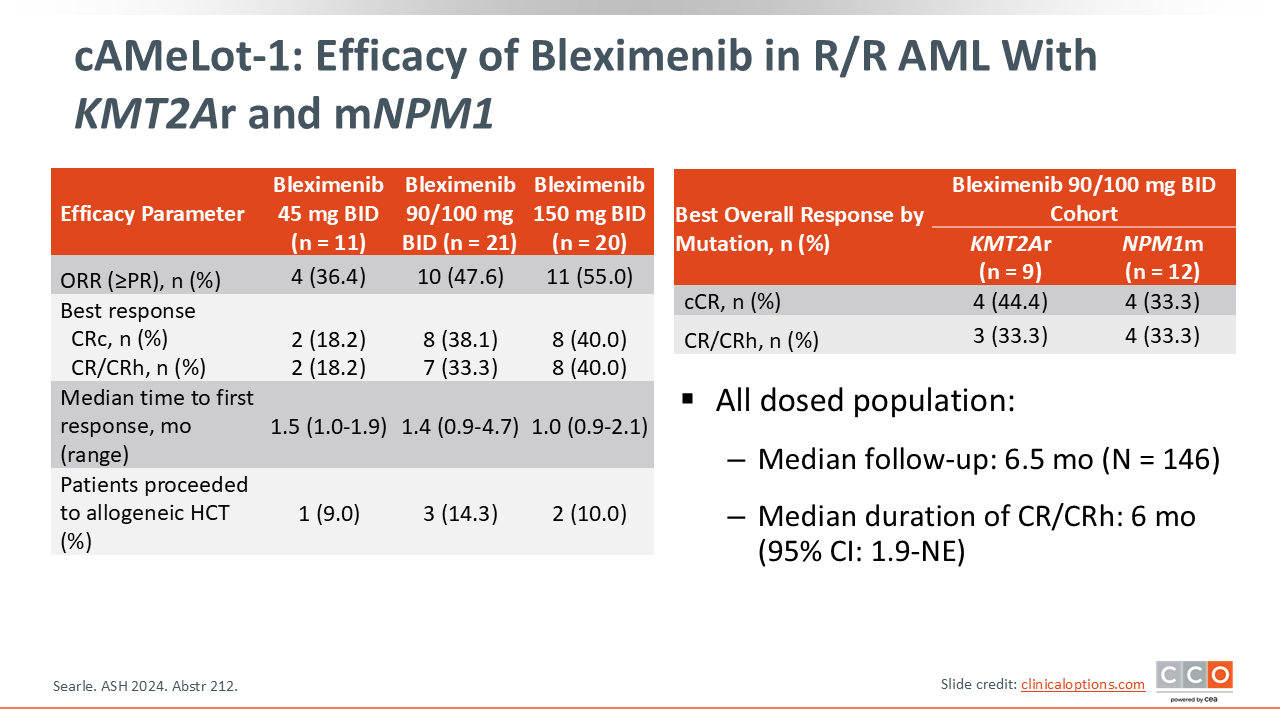
cAMeLot-1: Efficacy of Bleximenib in R/R AML With KMT2Ar and mNPM1
Eunice Wang, MD:
The RP2D of bleximenib was 100 mg twice daily. The median duration of CR/CRh with bleximenib monotherapy in R/R AML was 6 months, which is very comparable to that previously reported for revumenib at 4.7 months and ziftomenib at 5.1 months. The CRc rate with bleximenib 100 mg was 38.1% and the CR plus CRh rate was 33.3%, with 14.3% of patients successfully proceeding to allogeneic HCT.22
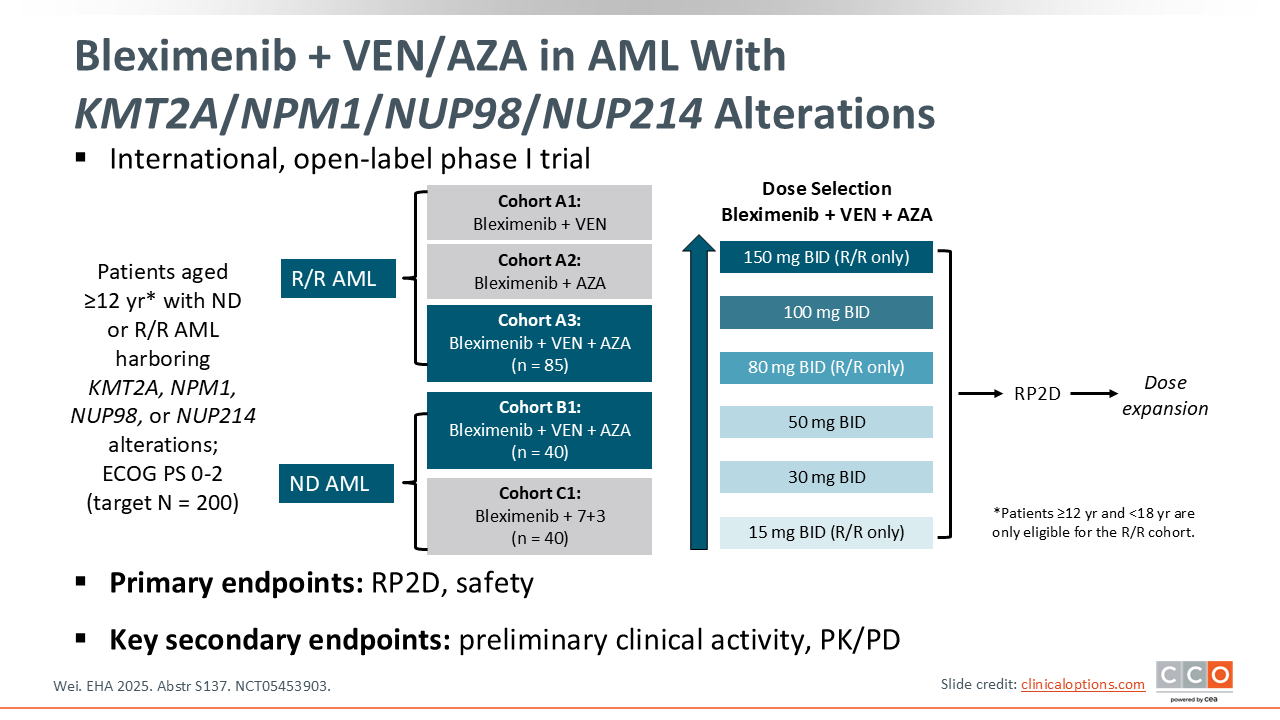
Bleximenib + VEN/AZA in AML With KMT2A/NPM1/NUP98/NUP214 Alterations
Eunice Wang, MD:
Bleximenib is also being evaluated in combination with venetoclax/azacitidine in newly diagnosed and R/R AML at the 100 mg twice daily dosing (NCT05453903).23
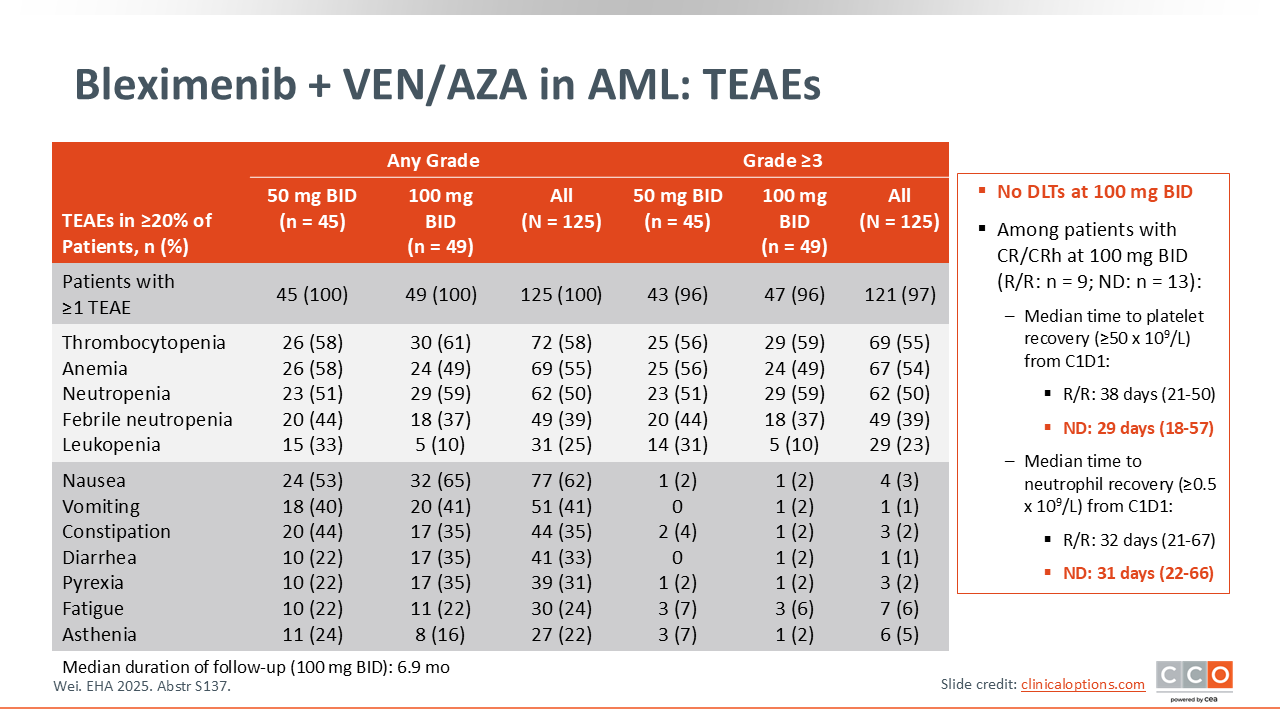
Bleximenib + VEN/AZA in AML: TEAEs
Eunice Wang, MD:
At the bleximenib 100 mg twice daily dose, there were no dose-limiting toxicities. The median time to platelet recovery varied between 29 days in newly diagnosed patients and 38 days in R/R patients. The regimen was well-tolerated with no significant additional AEs in the combination regimen. The incidence of DS appeared to be lower with the venetoclax/azacitidine combination as only 4% of the patients experienced grade ≥3 DS. No significant QTc prolongation was reported, with all events being grade 1 and not requiring dose interruptions.23
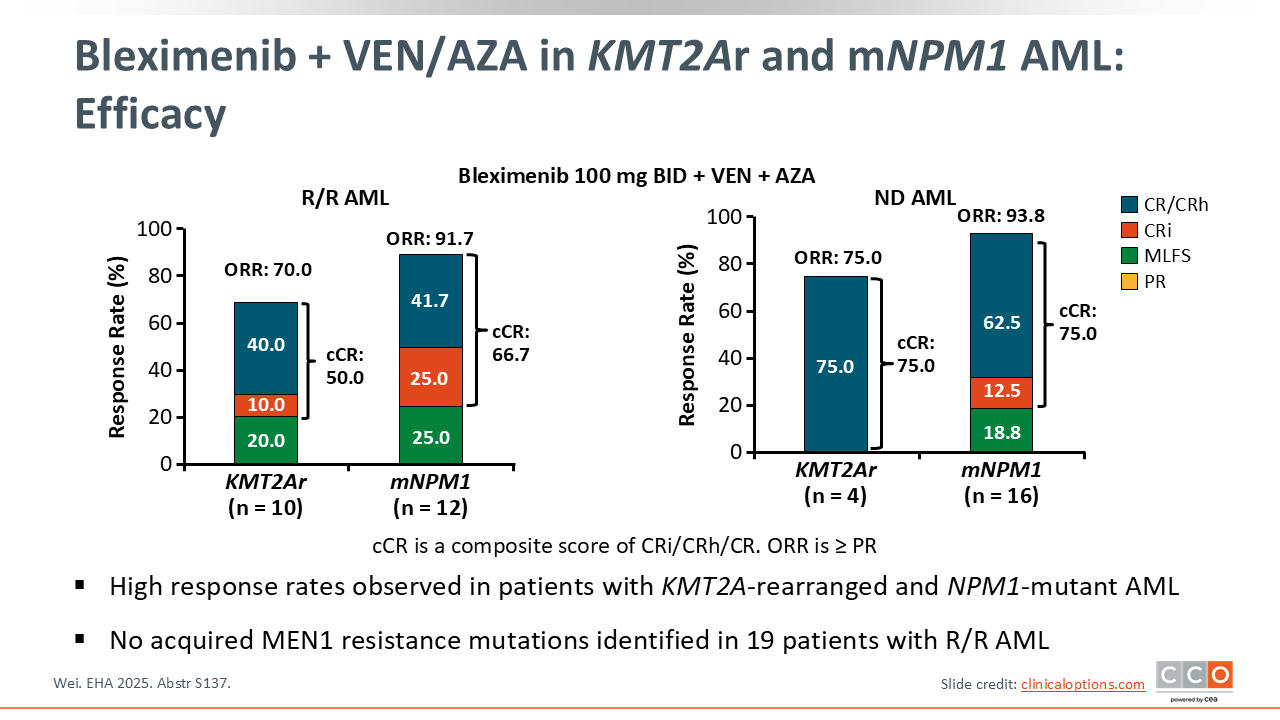
Bleximenib + VEN/AZA in KMT2Ar and mNPM1 AML: Efficacy
Eunice Wang, MD:
In a small number of patients with AML treated in the newly diagnosed setting, early results of bleximenib plus chemotherapy regimens have been impressive. The combination of bleximenib with venetoclax and azacitidine yielded an ORR of 93.8% among 16 patients with mNPM1 with 75% achieving a CRc. In 4 patients with newly diagnosed AML and KMT2Ar, the ORR and CRc were 75%. Similarly in patients with R/R AML, the 12 patients with mNPM1 experienced an ORR of 91.7% and CRc of 66.7% while 10 patients with KMT2Ar experienced an ORR of 70% and a CRc of 50%.23
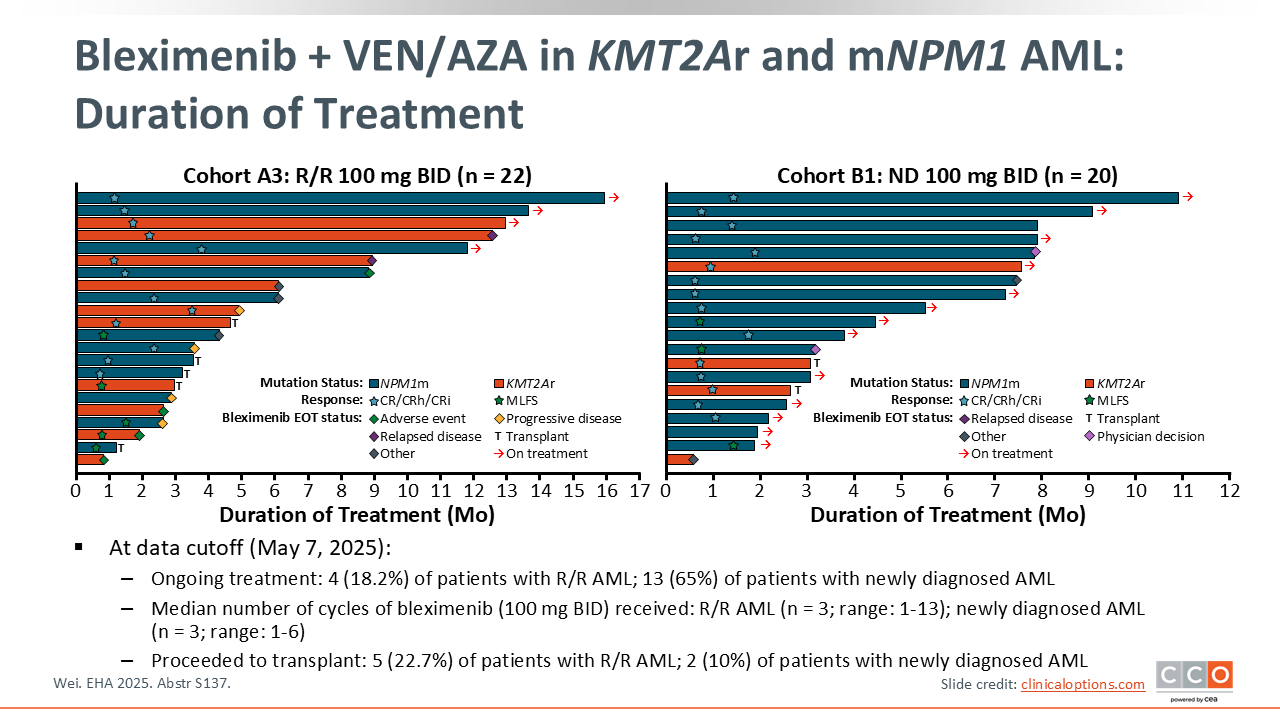
Bleximenib + VEN/AZA in KMT2Ar and mNPM1 AML: Duration of Treatment
Eunice Wang, MD:
Patients on bleximenib/venetoclax/azacitidine experienced long duration of treatment with 65% of newly diagnosed patients still receiving ongoing treatment as of the data cutoff on May 7, 2025. Seven patients proceeded to subsequent allogeneic HCT, 2 patients from the ND cohort and 5 patients from the R/R cohort.23
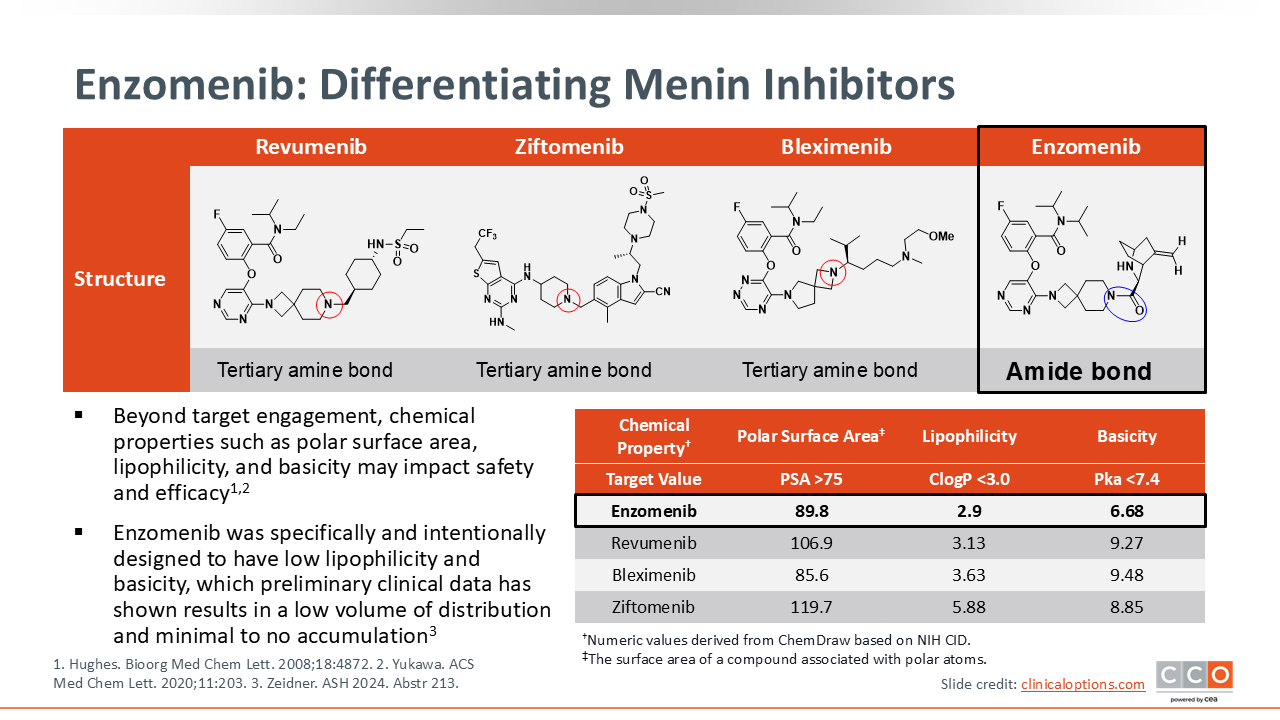
Enzomenib: Differentiating Menin Inhibitors
Eunice Wang, MD:
The last menin inhibitor we will discuss is enzomenib. Enzomenib is a new-generation menin inhibitor with a unique chemical structure from other menin inhibitors due to the presence of an amide bond. The structure was specifically chosen for further clinical development because of chemical properties such as low lipophilicity and basicity, which may lead to a low volume of distribution and low tissue accumulation. These properties were hypothesized to result in less extramedullary symptoms and potentially less DS, which is common with menin inhibitors.24-26
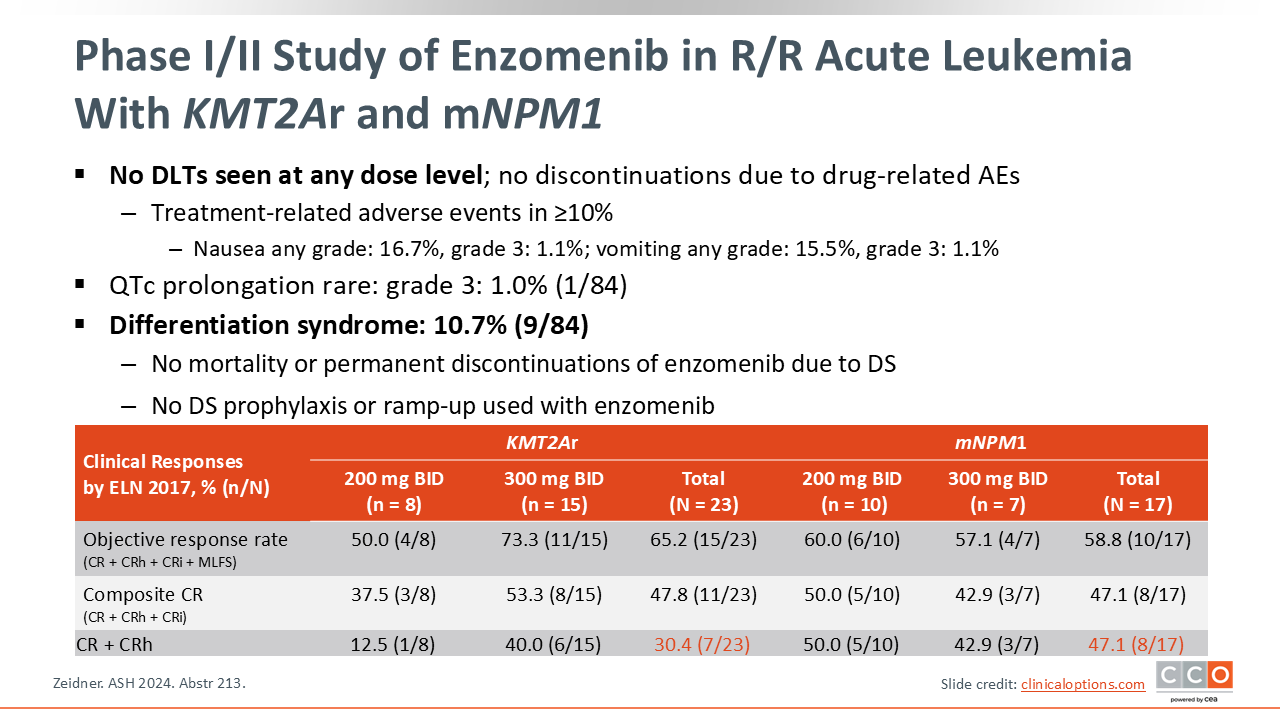
Phase I/II Study of Enzomenib in R/R Acute Leukemia With KMT2Ar and mNPM1
Eunice Wang, MD:
In the first-in-human phase I trial with enzomenib, there has been no reported dose-limiting toxicity identified, including no dose-limiting QTc prolongation, and no dose-limiting DS. DS was reported at approximately half the rate (10.7%) reported with other menin inhibitors (approximately 20%-30%), and patients receiving enzomenib did not require any DS prophylaxis with corticosteroids. If confirmed, this might be a distinguishing factor of enzomenib from other menin inhibitors.
In early studies, enzomenib therapy resulted in similar rates of clinical responses as the other menin inhibitors in the same patient populations. The reported CR plus CRh rate was 30.4% and 47.1% in KMT2Ar and mNPM1 patients, respectively, and the ORR was ≥50%. Currently, enzomenib is also now planned to be studied in combinatorial studies to investigate if it can be combined with, for example, a venetoclax/azacitidine backbone similar to other menin inhibitors.24
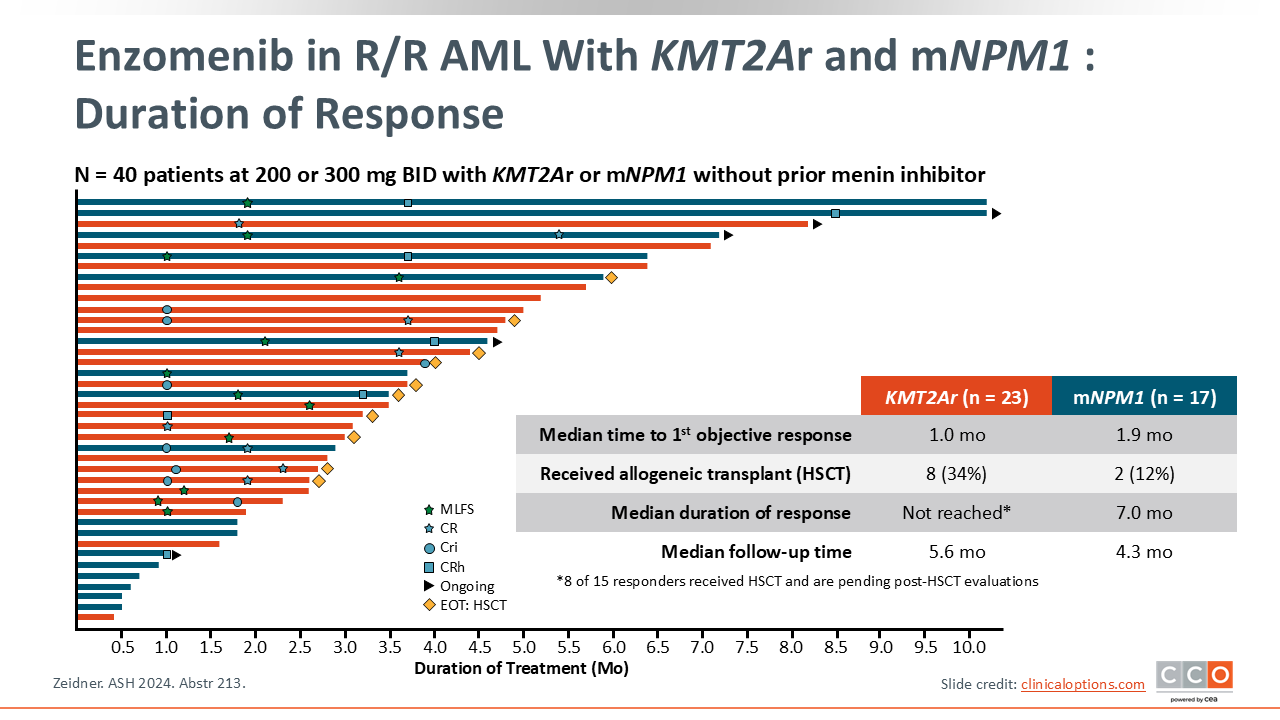
Phase I Enzomenib: Duration of Responses
Eunice Wang, MD:
The median time to objective response for enzomenib was 1.0 month for patients with KMT2Ar disease and 1.9 months for patients with mNPM1. This short time frame is potentially due to the tissue distribution of enzomenib. With a very short follow-up, the median DoR was not reached for the KMT2Ar group and was 7.0 months for the mNPM1 group.24
Resistance to Menin Inhibitors: Somatic Menin Mutations Develop With Revumenib Therapy
Eytan Stein, MD
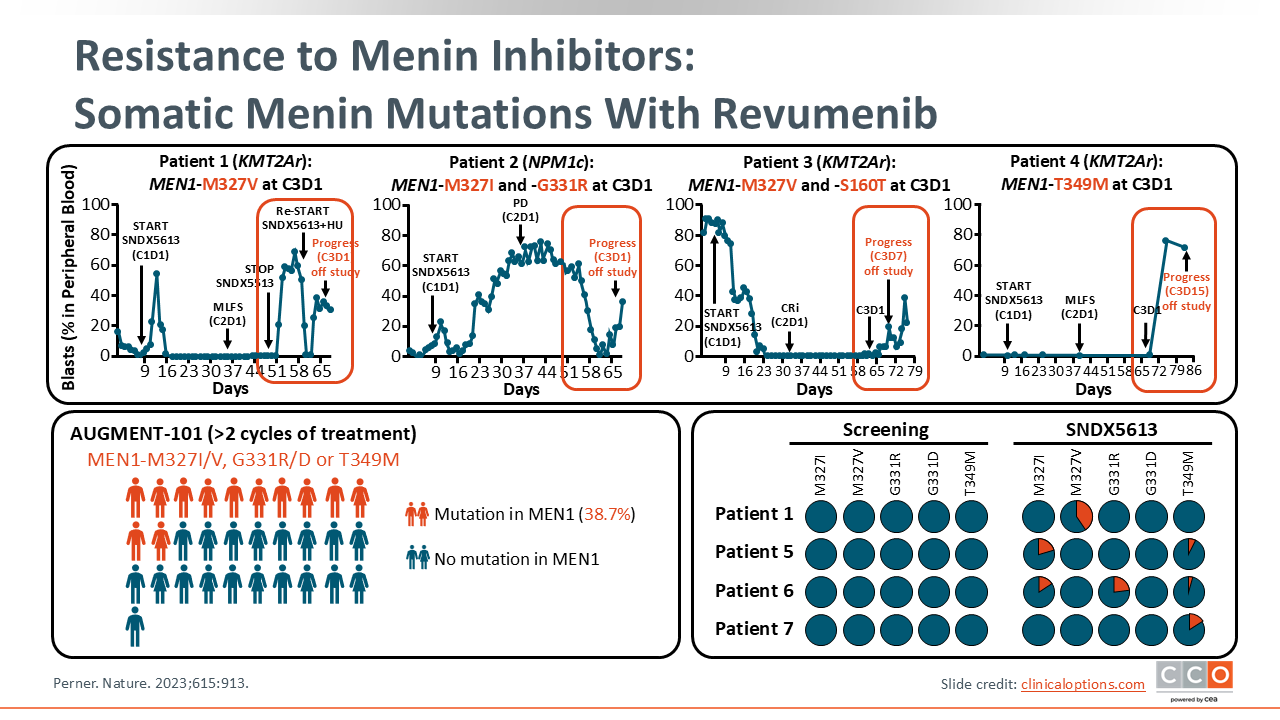
Now we will discuss resistance to menin inhibitors. We noticed early on that patients would respond but relapse quickly after receiving revumenib. At Memorial Sloan Kettering, the MEN1 gene is on our MSK-IMPACT mutation panel. This allowed us to identify mutations in MEN1 which prevented revumenib from binding to menin.
Of interest, when we interrogated all of our patient samples, we found 40% of patients at some point harbored a MEN1 mutation in the binding pocket for revumenib, regardless of whether they had clinically relapsed.
There are data that demonstrated that each menin inhibitor binds to the menin protein with different binding patterns.27 Through CRISPR analysis, researchers determined that different menin inhibitors are likely to cause potentially drug-specific mutations. Even though menin mutations were initially identified in patients exposed to revumenib, it is possible that each menin inhibitor may also result in a specific pattern of resistance mutations.
This may already be being witnessed in the clinic with newer menin inhibitors. For example, bleximenib resistance mutations may be starting to be identified.
Using CRISPR technology, menin-resistant mutations could be determined and treatment algorithms tailored accordingly.
None of these menin mutations are currently available in commercial assays, but this is an intriguing thought moving forward as we think about the management of our patients with R/R AML and mNPM1 or KMT2Ar.
Clonal Evolution, and Considerations for Treatment Selection
Eunice Wang, MD:
As menin inhibitors move into the frontline setting and we start to consider them as the next targeted therapy, it is important to determine strategies to identify candidates for these agents in both the newly diagnosed and R/R disease settings.
The diagnostic workup is key for identifying these individuals as we continue to pursue progress through clinical trial investigation. At our center, we have a multifaceted strategy that is recommended and advocated by the NCCN and other groups.5,28
If we have a patient who we suspect has AML with peripheral blasts or severe pancytopenias, we will collect peripheral blood. If there are peripheral blasts, we will send the sample for analysis. If no peripheral blasts, our practice is to perform bone marrow biopsies with ideally same-day morphology and immunohistochemistry results to confirm tumor cell lineage, ie, lymphoid vs myeloid. We also perform same or next day marrow flow cytometric analysis for myeloid and lymphoid markers.
Within 5-7 days, we ideally have conventional cytogenetic and targeted FISH results.
Our pathologists perform cytogenetics specifically looking for a translocation of 11q23 with another gene. We also order a pan-myeloid or pan-hematologic myeloid next-generation sequencing (NGS) assay with a 3-5 day turnaround which, provides results of an array of gene mutations, including FLT3, IDH1, IDH2, TP53, as well as secondary mutations, and NPM1.
For healthcare professionals with limited access or longer turnaround for an NGS panel, using a qualitative PCR or PCR test for mNPM1 may be helpful for quicker results to identify patients that could be eligible for a clinical trial of a frontline menin inhibitor.
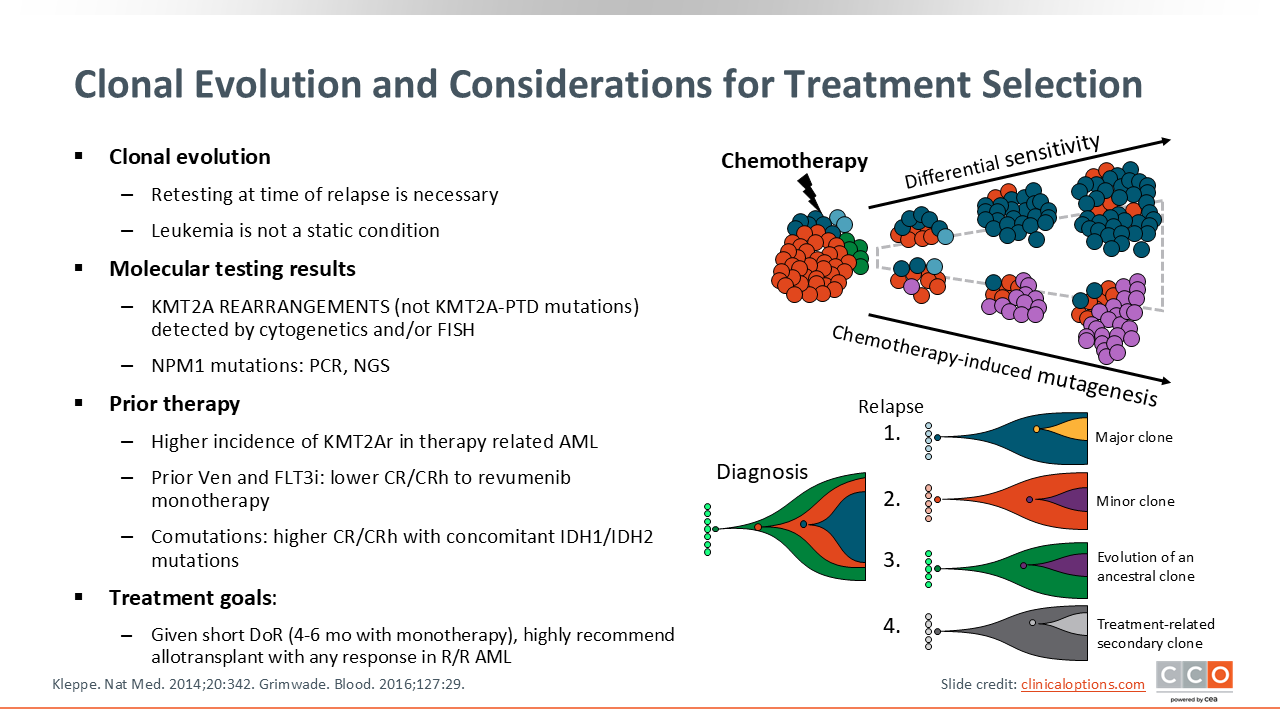
It is important that this type of testing occurs at the time of diagnosis as well as at relapse because prior treatment with intensive chemotherapy can select for different clones over time, leading to different mutational profiles prior to and following therapy. Therefore, it is essential to repeat the entire analysis, including cytogenetic analysis and NGS profiling at the time of disease recurrence.29
Highly sensitive NPM1 qualitative PCR can be used reliably for MRD testing. At our center, we also use a multiparameter flow cytometric assay for patients that do not have an MRD molecular marker (ie, KMT2Ar) to monitor responses to therapy. We recommend these analyses for patients.
I want to emphasize a couple of key points to remember.
First, there is a higher incidence of KMT2Ar in patients with prior therapy related to acute leukemias. The presence of comutations, particularly with mNPM1 AML, can be helpful for treatment selection including future combinatorial regimens. For example, patients with concomitant IDH1/IDH2 and mNPM1 have responded well to single-agent menin inhibitor therapy in the phase II studies reported to date with revumenib and ziftomenib. In addition, there is a possibility of future clinical trials combining FLT3 inhibitors as well as menin inhibitors for newly diagnosed patients with both FLT3 and NPM1 mutations. When giving these targeted therapies, it is important to have allogeneic HCT available once you start therapy in the R/R setting as a strategy to achieve long-term efficacy considering the short DoR generally seen with these inhibitors.
Incidence and Severity of DS across MI clinical trials
Eunice Wang, MD:
Finally, it is important to remember that menin inhibitors are associated with DS, which can have serious consequences for our patients. DS usually occurs in the first cycle with the initiation of menin inhibitor therapy. It is characterized by increased WBC count, fluid retention, and development of pleural/pericardial effusion, which are also evidenced clinically by respiratory distress and chest pain. Patients develop diffuse rashes and can have fevers and renal failure in severe cases. The median time to presentation of DS can be as short as 3-5 days and up to 8-10 days after initiation of therapy.
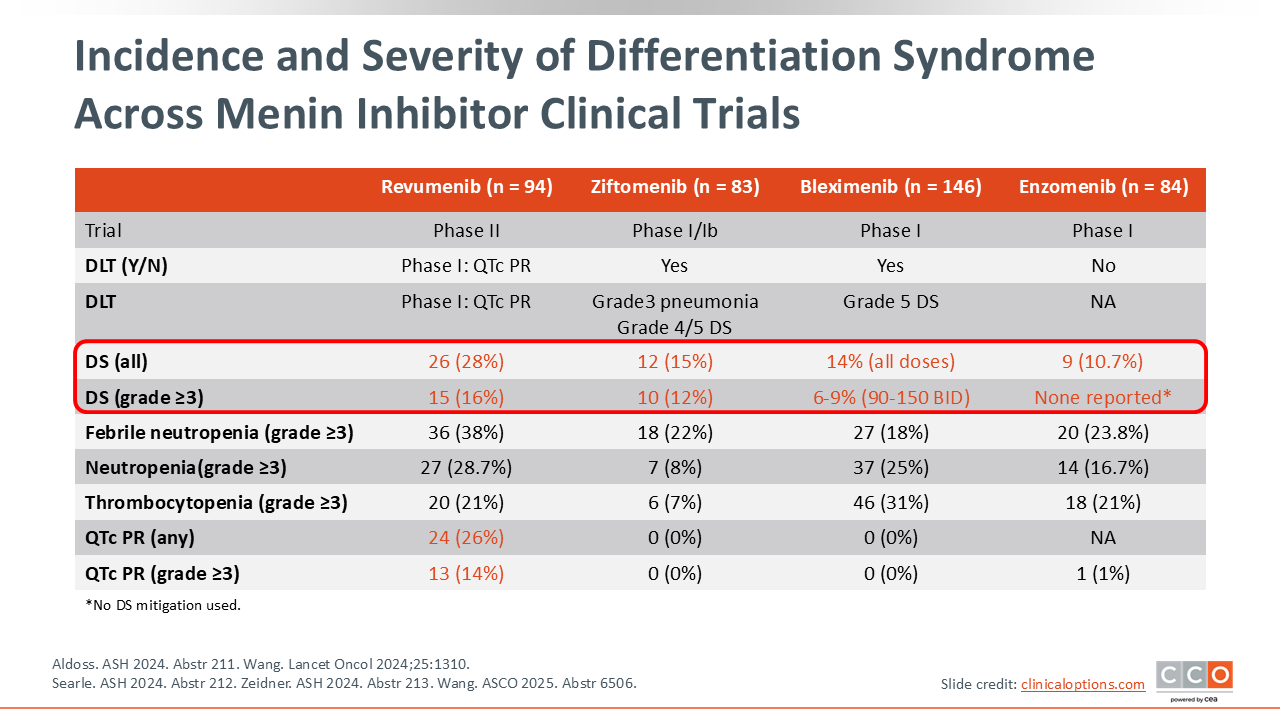
Treatment and prophylaxis of DS can be important. Across the menin inhibitor trials, we see DS rates of 10.7% to 28%. Grade 3 DS with mitigation strategies has been reduced to approximately 12% to 16%. However, management really involves early recognition of patients at high risk of disease.16,18,22,30,31
WBC counts must be brought under 20,000 at the time of menin inhibitor initiation. Cytoreduction with hydroxyurea or cytarabine can achieve lower WBC counts. If there are increasing signs or symptoms or even an increasing leukocytosis, patients may need to be monitored in an inpatient setting.
In the inpatient setting, patients who need cytoreduction prior to therapy should be put on prophylactic steroids with the initiation of the menin inhibitor. Also, if mitigation and supportive care strategies, including management of tumor lysis and DIC, do not quickly resolve in DS, then the menin inhibitor should be held until better clinical control is achieved. With appropriate mitigation strategies, DS is a manageable side effect. Although DS can be fatal in patients with AML, we do not withhold treatment of this highly curable cancer as a result.
Eytan Stein, MD:
To conclude, menin inhibitors are extraordinarily promising in the treatment of patients with acute leukemias and mNPM1 or KMT2Ar. However, there are a number of issues that need to be addressed as these therapies move into the clinic. First, what are we going to do about resistance mutations? The DoR with menin inhibitors as single agents is relatively short. Because of this short duration, we need to discover how to overcome resistance. This may require developing better menin inhibitors with unique types of resistance liabilities. Perhaps of more importance, we need to combine menin inhibitors with other drugs with different mechanisms of action and/or fewer resistance mechanisms. This combination strategy is already underway.
Second, we need to establish proper sequencing of menin inhibitors in our treatment paradigm for acute leukemias. For example, initial therapy may be standardized for 1 agent, but if patients develop specific resistance mutations, other drugs may be needed.
Third, we need to determine the efficacy of using menin inhibitors for patients who have already undergone an allogeneic HSCT. Is this something that is going to be safe to do? Is the myelosuppression associated with menin inhibitors going to be an issue in this setting? Also, will this approach benefit patients? We sometimes assume that maintenance therapy after allogeneic HSCT is beneficial, but I think that needs to be proven in a randomized study.
Finally, combining menin inhibitors with other targeted therapies is something that is being investigated now, but it is something with which we need more experience. Are we going to have specific algorithms for patients with co-occurring FLT3, IDH, and NPM1 mutations? Are we going to be administering complicated regimens like induction chemotherapy with 7+3, and a FLT3 inhibitor, an IDH inhibitor, and a menin inhibitor in attempts to induce patients into the deepest remission possible? Perhaps then removing some of those drugs to transition to maintenance therapy? Overall, we are making progress to help our patients with acute leukemias. I am hopeful that these questions will be answered over the next few years as we continue to make progress towards improving our patients’ outcomes.