CE / CME
ABIM MOC: maximum of 0.75 Medical Knowledge MOC point
Physicians: Maximum of 0.75 AMA PRA Category 1 Credit™
Released: July 31, 2025
Expiration: January 30, 2026
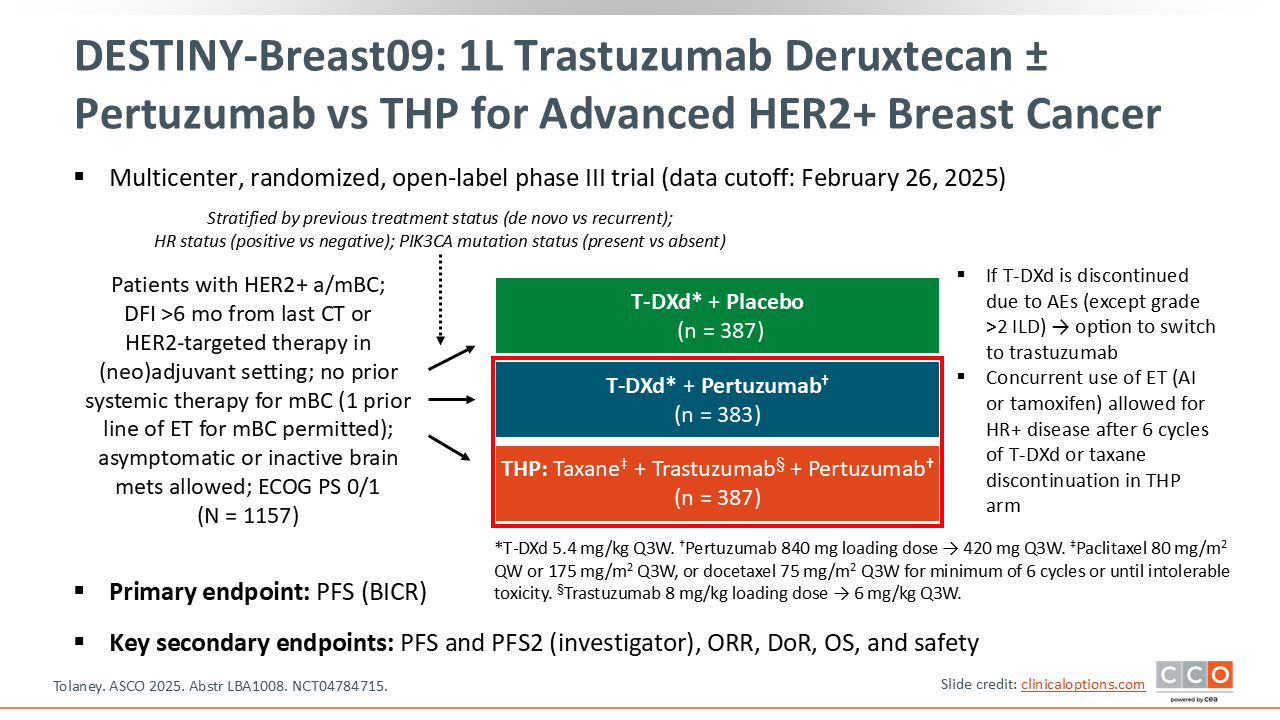
DESTINY-Breast09: 1L Trastuzumab Deruxtecan ± Pertuzumab vs THP for Advanced HER2+ Breast Cancer
Sara M. Tolaney, MD, MPH: The first study we will discuss is DESTINY-Breast09. This trial sought to understand whether T-DXd could have a role in first-line therapy for metastatic HER2-positive breast cancer. T-DXd has dramatically improved outcomes for patients with previously treated metastatic HER2-positive disease and is currently FDA approved as a second-line SoC based on DESTINY-Breast03, which demonstrated an unprecedented median PFS of 29 months.1
THP is the current first-line SoC and is associated with a median PFS of approximately 19 months.2 There was considerable interest in assessing T-DXd in the frontline setting.
DESTINY-Breast09 was a phase III study that randomized patients with metastatic HER2-positive breast cancer that was not previously treated with systemic therapy to T-DXd alone, T-DXd plus pertuzumab, or THP.3 Patients who were randomized to the T-DXd–containing arms were treated with T-DXd until disease progression. If T-DXd had to be discontinued early due to toxicity, then trastuzumab could be added, which was given alone in the T-DXd plus placebo arm or in combination with pertuzumab in the T-DXd plus pertuzumab arm. For those patients on the THP arm, the taxane had to be administered for a minimum of 6 cycles or until development of toxicity. For patients who had HR-positive disease, ET could be added either after a minimum of 6 cycles of T-DXd or after taxane discontinuation.
The primary endpoint was PFS, comparing T-DXd and pertuzumab to THP and comparing T-DXd and placebo to THP. This study was not powered to compare the 2 T-DXd–containing arms.
At ASCO 2025, the results from the interim analysis comparing T-DXd plus pertuzumab to THP were presented. This was because the T-DXd plus pertuzumab arm reached superiority at the time of the interim analysis based on the very stringent criteria that were set for interim success. The T-DXd alone arm did not meet the criteria set for superiority at the time of the interim analysis. That arm remains blinded and those patients continue to be followed. We will not see data from that arm until the final PFS analysis.
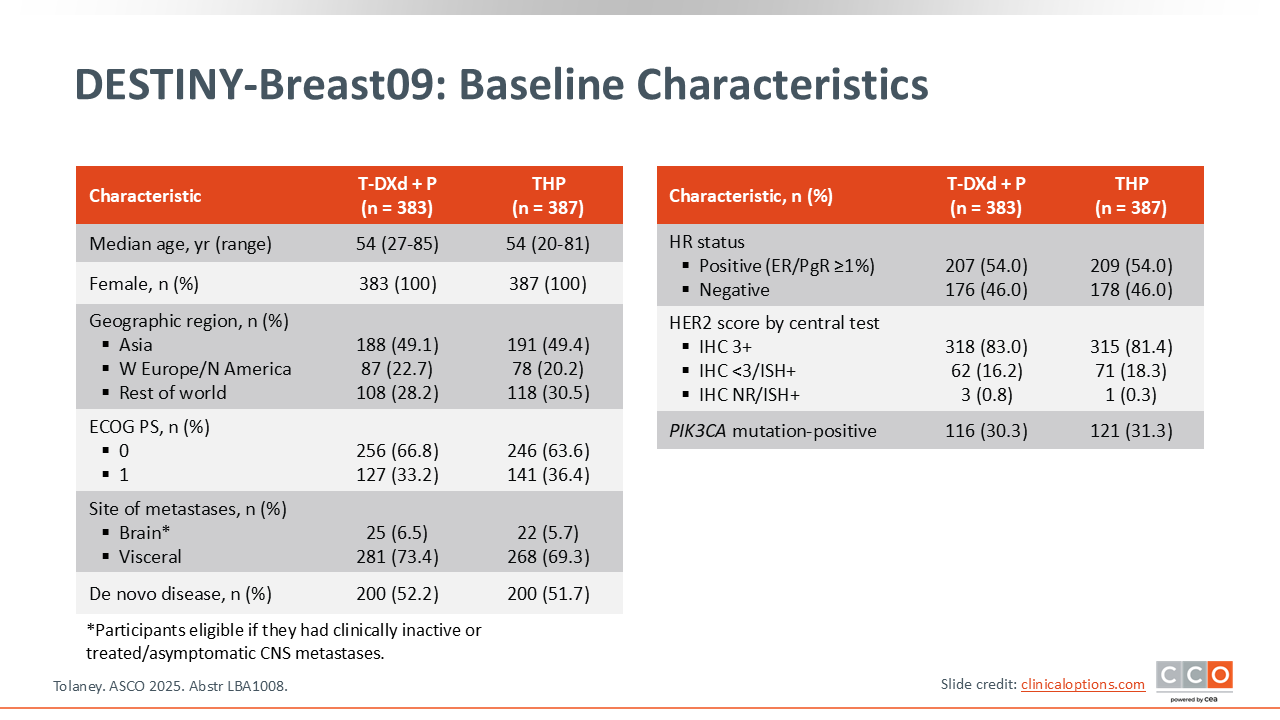
DESTINY-Breast09: Baseline Characteristics
Sara M. Tolaney, MD, MPH: Looking at the patients that were enrolled into the trial, a little more than 50% had de novo metastatic disease and the vast majority of patients had visceral metastases.
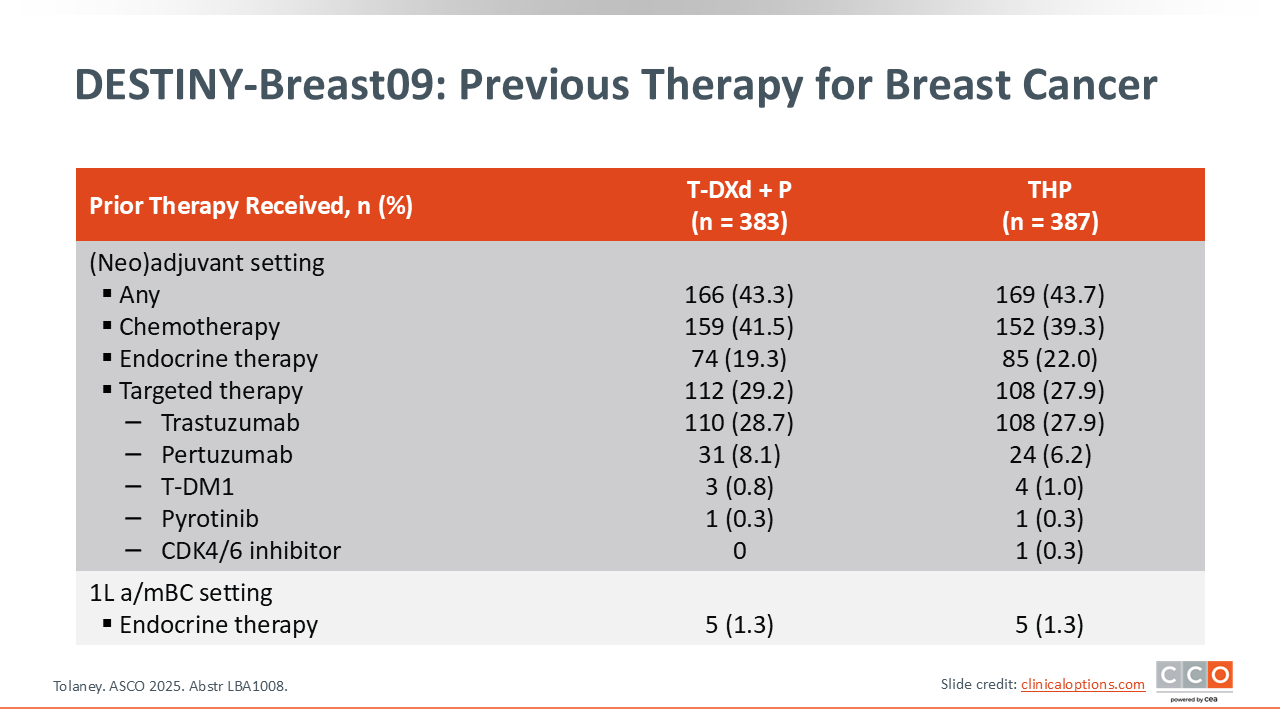
DESTINY-Breast09: Previous Therapy for Breast Cancer
Sara M. Tolaney, MD, MPH: Approximately half of the patients had systemic therapy in the early disease setting. When you look at the types of therapy received in the early disease setting, it is notable that approximately 28% of patients received prior trastuzumab, approximately 7% prior pertuzumab, and 1% prior T-DM1.
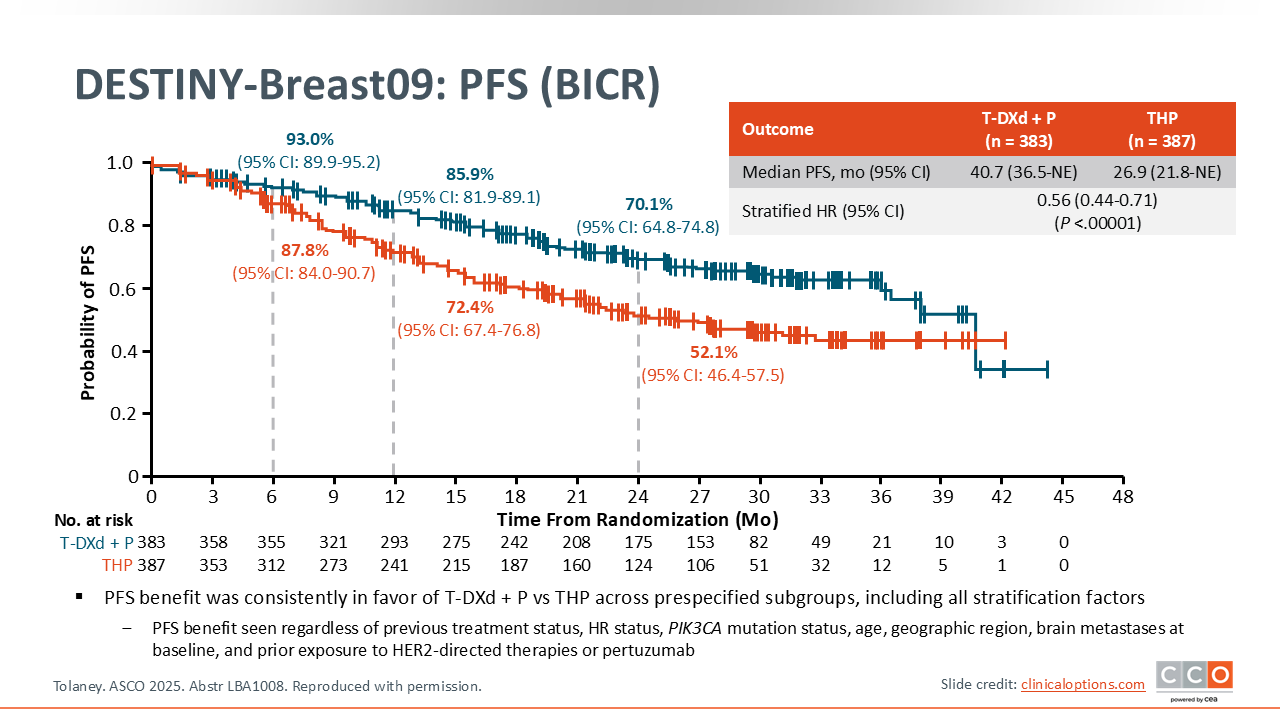
DESTINY-Breast09: PFS (BICR)
Sara M. Tolaney, MD, MPH: Looking at the primary endpoint of PFS, the combination of T-DXd and pertuzumab was associated with a statistically significant and clinically meaningful improvement in PFS, with a median of 40.7 months for T-DXd and pertuzumab compared with 26.9 months for THP. This is consistent with the hazard ratio of 0.56 and a P value <.00001. This was a very striking difference between the 2 arms.
One thing I would point out is that when you look at the curves, you can see that they do separate very early. When you look at the 6-month landmark analysis, you can see that at 6 months, approximately 12% of patients had already progressed on THP, whereas you see about half as many patients had progressed on the T-DXd and pertuzumab arm. Over time, the curves continue to widen and separate, but there is considerable instability in the tail of the curve. Keep in mind that the median follow-up at this interim analysis was 29 months, so there are very few events at the tail of the curve, which is causing this instability. We do know that currently, 46% of patients on the T-DXd plus pertuzumab arm are still receiving treatment. This suggests that the median PFS is likely to evolve with further follow-up.
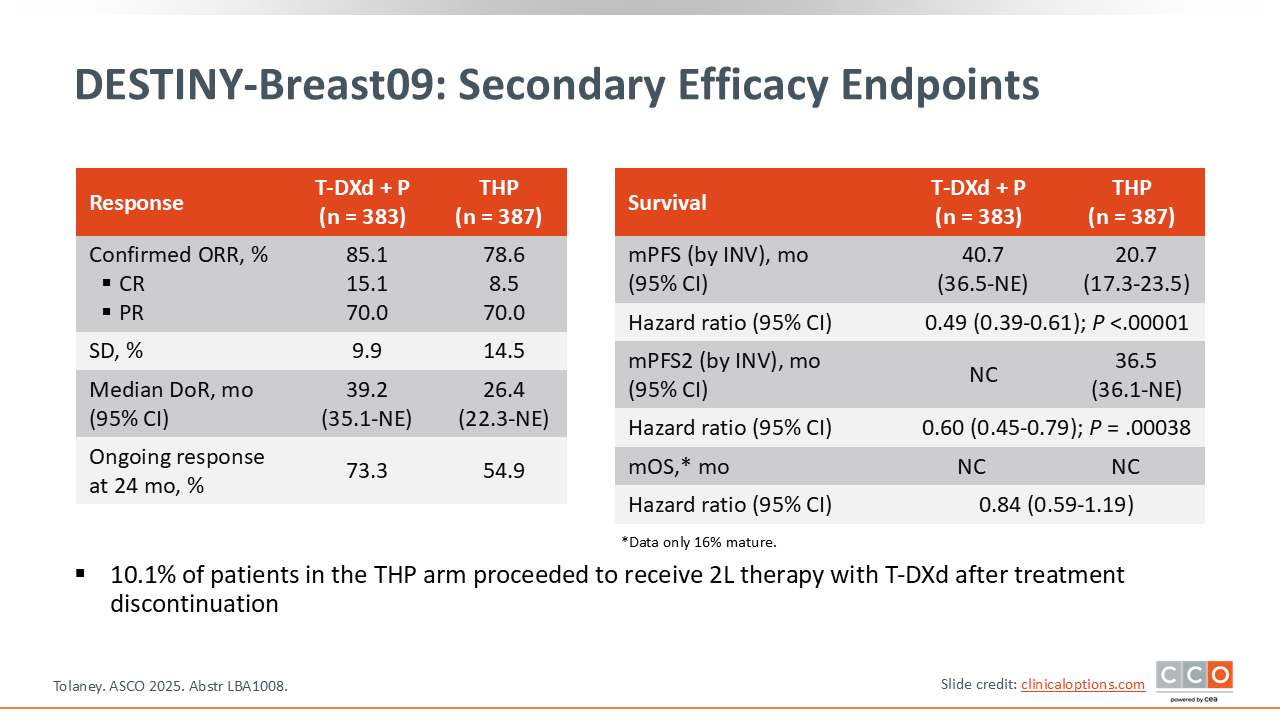
DESTINY-Breast09: Secondary Efficacy Endpoints
Sara M. Tolaney, MD, MPH: Looking at secondary efficacy endpoints, the ORR was numerically higher with T-DXd plus pertuzumab compared with THP, and the complete response (CR) rate was almost double, at 15% with T-DXd plus pertuzumab vs 8.5% with THP. Of importance, responses were substantially more durable with T-DXd plus pertuzumab, where the median DoR was 39.2 months compared with 26.4 months for THP.
One thing to keep in mind is that the overall survival (OS) data are still very immature, as only 16% of survival events had occurred at the time of the interim analysis. There was a slight trend for survival benefit with T-DXd plus pertuzumab with a hazard ratio of 0.84. But because the OS data are so immature, it was important to also look at PFS2, which is defined as the time from randomization to time of progression on second-line therapy. The hazard ratio for PFS2 was 0.6, again favoring T-DXd plus pertuzumab.
One of the questions that arises when you look at PFS2 is what therapies patients are receiving in that second-line setting. Of note, of patients in the control arm who had discontinued THP and then went on to receive a second line of treatment, 10% received T-DXd as their second-line treatment and 12% received T-DM1.
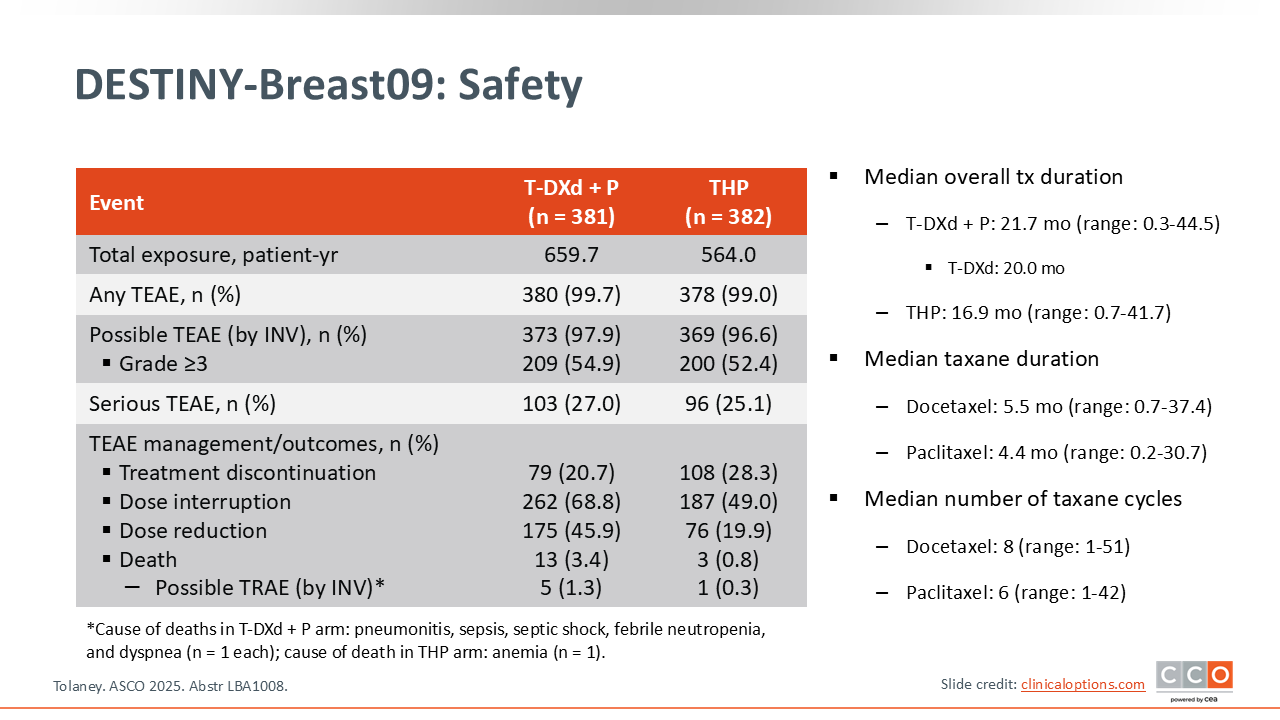
DESTINY-Breast09: Safety
Sara M. Tolaney, MD, MPH: Looking at safety, the duration of therapy was substantially longer with T-DXd plus pertuzumab at approximately 22 months compared with approximately 6 months of cytotoxic therapy in the THP arm. Despite thelonger duration of cytotoxic treatment with T-DXd plus pertuzumab, the rate of grade 3/4 TEAEs and the rate of serious TEAEs was actually similar between the 2 arms. There were more dose reductions and dose delays with T-DXd plus pertuzumab compared with THP. There were also more possible treatment-related deaths with T-DXd plus pertuzumab vs THP (5 vs 1).
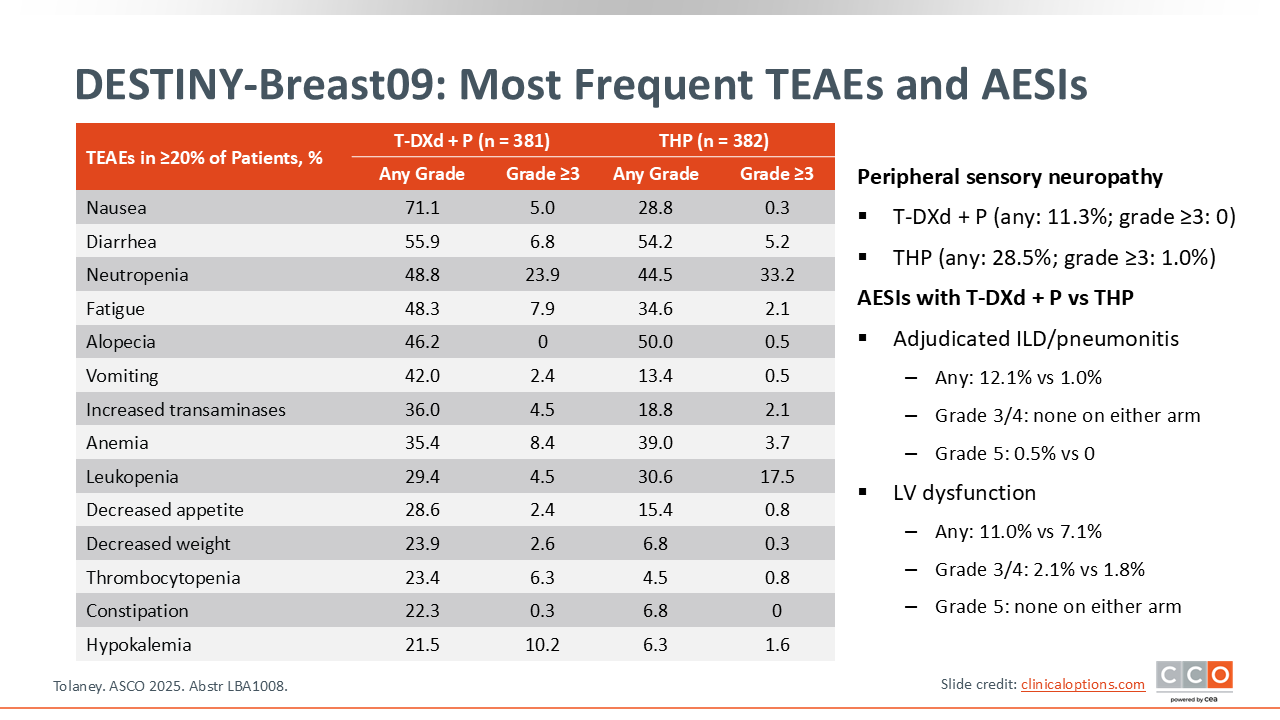
DESTINY-Breast09: Most Frequent TEAEs and AESIs
Sara M. Tolaney, MD, MPH: Looking at the most common adverse events (AEs) by arm, these are very consistent with what we already know to be toxicities from these agents, with nausea, diarrhea, neutropenia common with T-DXd plus pertuzumab, and diarrhea, neutropenia, and anemia common with THP. The rate of interstitial lung disease (ILD) was 12% with T-DXd plus pertuzumab, with the majority of events being low grade. There were 2 grade 5 ILD events that occurred with T-DXd plus pertuzumab. The rate of left ventricular dysfunction was numerically higher with T-DXd plus pertuzumab compared with THP.
DESTINY-Breast09: Conclusions
Sara M. Tolaney, MD, MPH: Overall, I think the DESTINY-Breast09 study showed us that giving T-DXd plus pertuzumab significantly improved PFS for patients with HER2-positive metastatic breast cancer (mBC) compared with the current SoC with THP. There was also a higher ORR and CR rate and the safety profile was consistent with the known toxicities of the agents in this study. I believe that T-DXd plus pertuzumab has the potential to become a new first-line SoC for patients with HER2-positive MBC.
Obviously, this is a different approach than how we currently treat our patients. We have become accustomed to the idea of using induction therapy with THP and then moving to HP maintenance. We have also seen things evolve recently with data from the PATINA trial showing that adding palbociclib to maintenance therapy with trastuzumab with or without pertuzumab plus ET improved PFS for patients with HR-positive disease.4 How do you think about this in our current treatment paradigm? Do you think T-DXd and pertuzumab should be utilized? Should it be utilized in select patients?
Kevin Kalinsky, MD, MS, FASCO: It is nice to see a drug that is so active in patients. I am not surprised by the efficacy that we are seeing in the first-line setting, considering what we have seen in later-line settings in this population. The side effect profile is similar to what we would have anticipated, so we are just waiting for data from the T-DXd alone arm.
Ultimately, I think that there are a number of questions that remain, including how we will think about some sort of induction approach similar to what was done in the CLEOPATRA trial of THP. For example, if you start with T-DXd plus pertuzumab, can you then take away the T-DXd and continue with HP? Could we apply a PATINA maintenance regimen for patients with HR-positive disease?
I think that there are some patients for whom I might continue T-DXd plus pertuzumab if this is available as an option. For example, those patients with significant visceral disease who still need a response, or patients with central nervous system metastasis. But I also think for other patients I might consider starting T-DXd plus pertuzumab for 6 cycles or so, and then if they are HR-positive, move to the PATINA regimen. If a patient with hormone-negative disease had a great response T-DXd plus pertuzumab, I might consider a maintenance regimen similar to what we do with THP. I am curious what you think.
Sara M. Tolaney, MD, MPH: I wish I had all the answers because this study does bring up so many questions. Here we only have data for patients receiving T-DXd plus pertuzumab until disease progression or toxicity requiring stoppage. I think what we would really love to understand is if we could get a patient to a CR or maximal response, could we then switch them over to maintenance—which was not done in DESTINY-Breast09—with the idea of trying to preserve QoL while maintaining response. I think that is really an open question.
There are studies that are ongoing to look at this question. For example, DEMETHER is a single-arm phase II study in which patients with previously untreated HER2-positive advanced breast cancer will receive 6 cycles of T-DXd followed by HP maintenance, with ET allowed in this setting.5
Practically speaking, I think most of us are going to want to use T-DXd plus pertuzumab simply because of the more robust efficacy. But I think people are going to want to better understand if there is an approach where maybe we do not have to continue this regimen until disease progression, and hopefully we will learn more as new studies emerge. It is good to have the potential to use this approach though.
Kevin Kalinsky, MD, MS, FASCO: I agree.
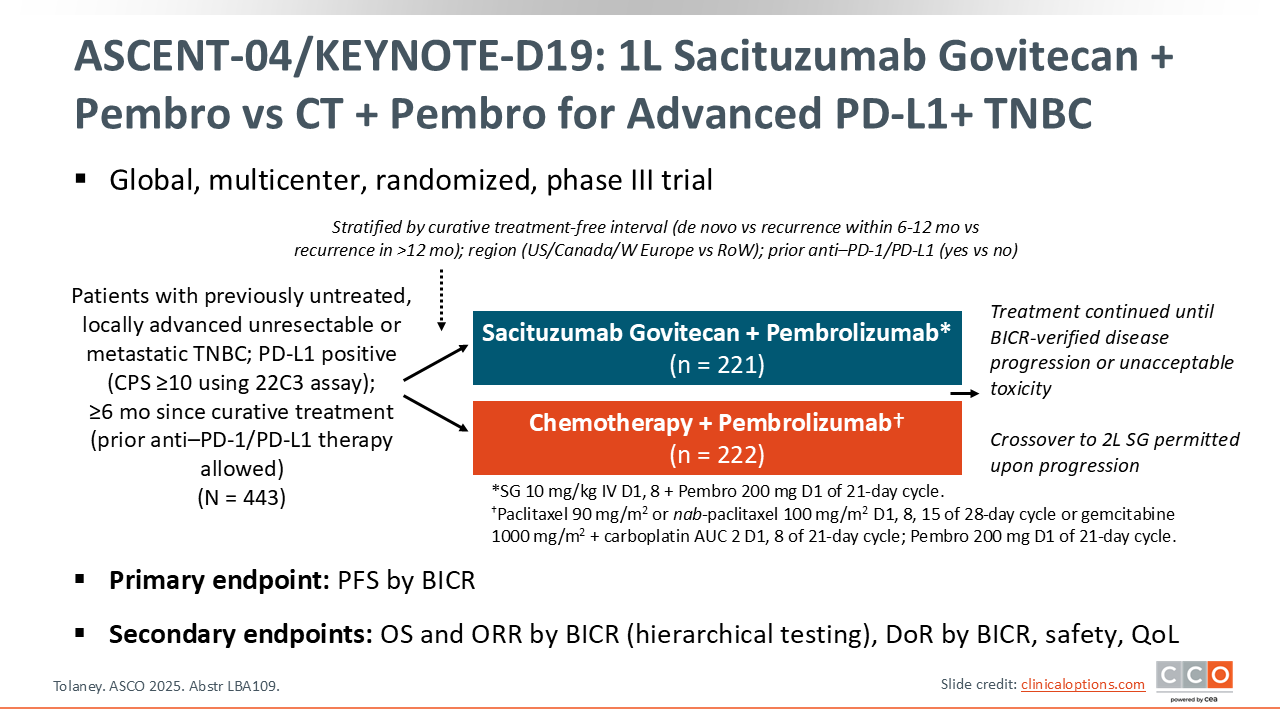
ASCENT-04/KEYNOTE-D19: 1L Sacituzumab Govitecan + Pembro vs CT + Pembro for Advanced PD-L1+ TNBC
Sara M. Tolaney, MD, MPH: Next, we will turn to triple-negative breast cancer (TNBC) to discuss the ASCENT-04 trial. This trial sought to understand whether the combination of sacituzumab plus pembrolizumab could be better than the current SoC chemotherapy plus pembrolizumab for patients who have previously untreated metastatic TNBC that is PD-L1 positive. KEYNOTE-355 established chemotherapy plus pembrolizumab as the current first-line SoC for patients with PD-L1–positive metastatic TNBC, but we have also seen how effective sacituzumab govitecan can be in the pretreated TNBC setting vs chemotherapy.6,7 We have also seen some interesting data to suggest that antibody–drug conjugates (ADCs) could work synergistically with checkpoint inhibition. This made the idea of looking at the combination of sacituzumab govitecan and pembrolizumab in this setting very attractive.
ASCENT-04 randomized patients who had not had any systemic treatment for metastatic, PD-L1–positive TNBC to sacituzumab govitecan plus pembrolizumab or chemotherapy plus pembrolizumab with a primary endpoint of PFS.8
ASCENT-04/KEYNOTE-D19: Baseline Characteristics
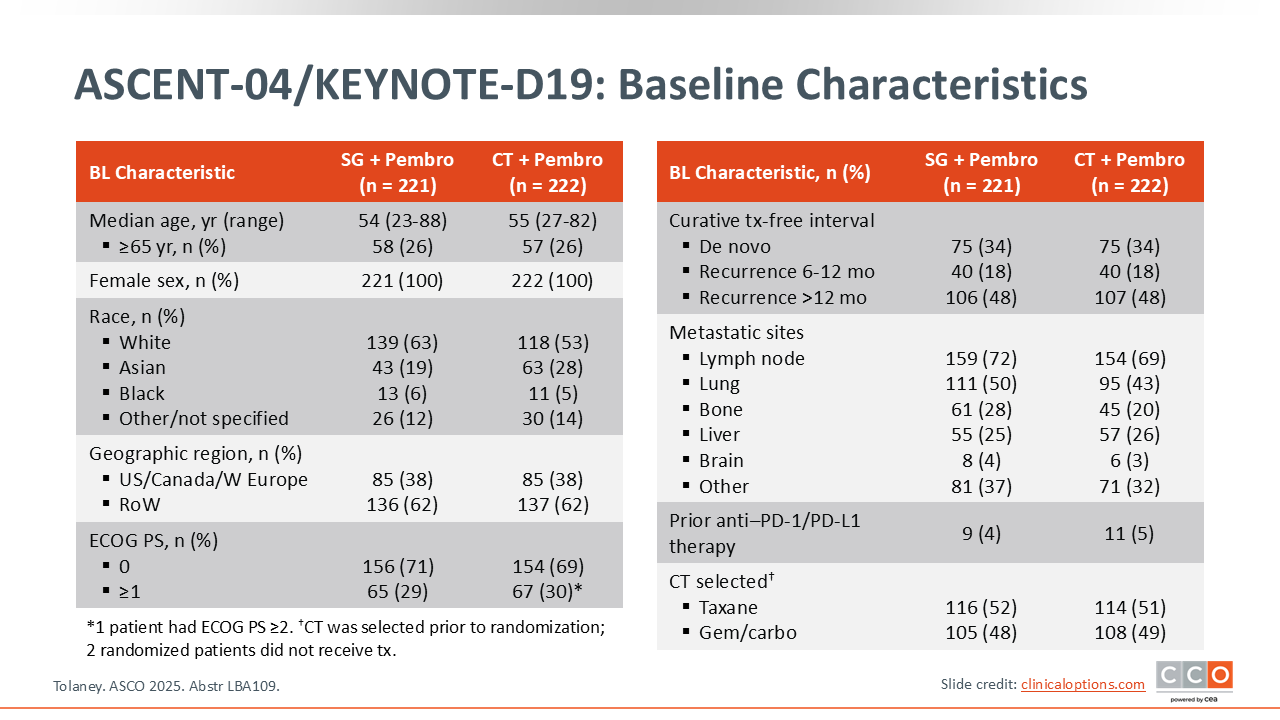
Sara M. Tolaney, MD, MPH: Of note, approximately a third of patients in this study had de novo metastatic disease. Approximately 20% of patients had recurred within 6-12 months of completion of systemic therapy in the early disease setting. Approximately half the patients had recurred more than 12 months from completion of systemic treatment.
The majority of patients did have visceral metastases, with half having lung metastases. Approximately 5% of patients had received an immune checkpoint inhibitor (ICI) in the early disease setting. This was allowed for this trial, as long as patients had at least 6 months from completion of any systemic treatment in the early disease setting. For the chemotherapy arm, patients had to select which chemotherapy drug they would choose if randomized to that arm before randomization. Approximately half of the patients elected to receive a taxane and half chose to receive gemcitabine plus carboplatin.
ASCENT-04/KEYNOTE-D19: PFS by BICR
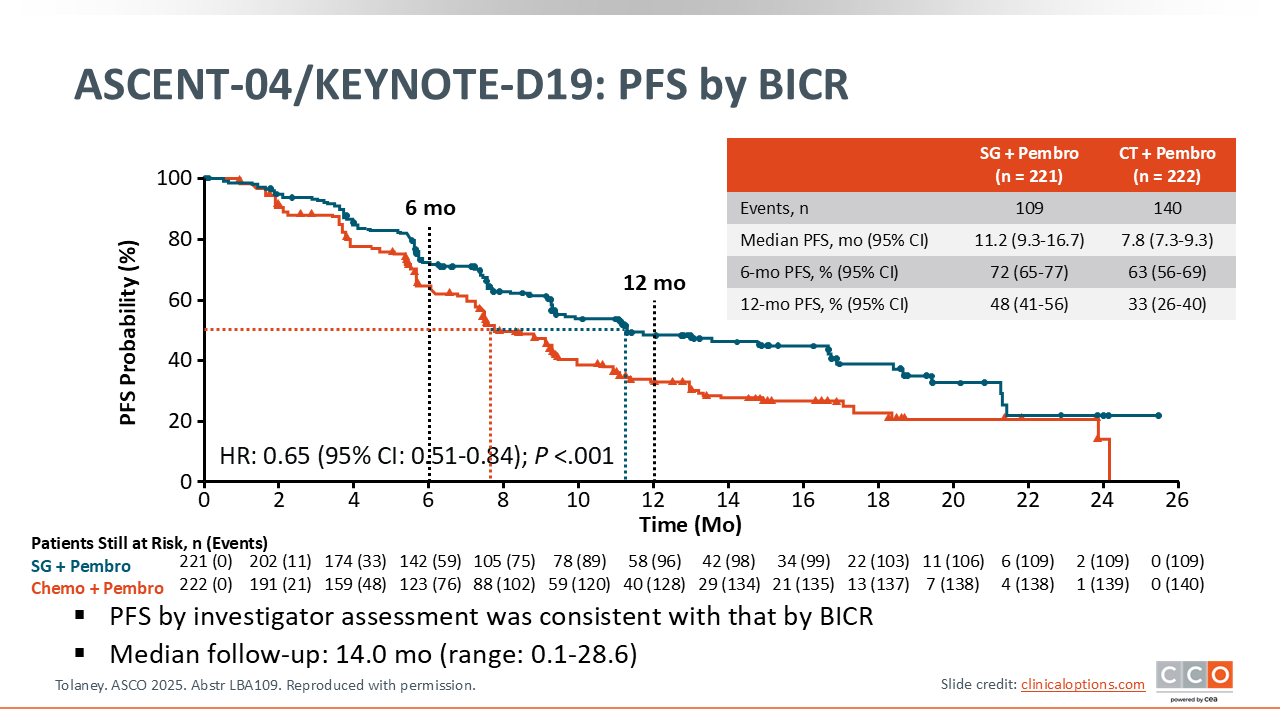
Sara M. Tolaney, MD, MPH: Here are the primary endpoint data for PFS. The combination of sacituzumab govitecan and pembrolizumab was associated with significant improvement in PFS compared with chemotherapy plus pembrolizumab (median PFS 11.2 vs 7.8 months; HR: 0.65; P <.001). This is a very robust difference of approximately 3.4 months between the 2 arms. This benefit was seen across all landmark time points where at 12 months, 48% of patients were free of disease progression or death with sacituzumab govitecan plus pembrolizumab arm vs 33% with chemotherapy plus pembrolizumab.
ASCENT-04/KEYNOTE-D19: PFS by BICR, by Subgroup
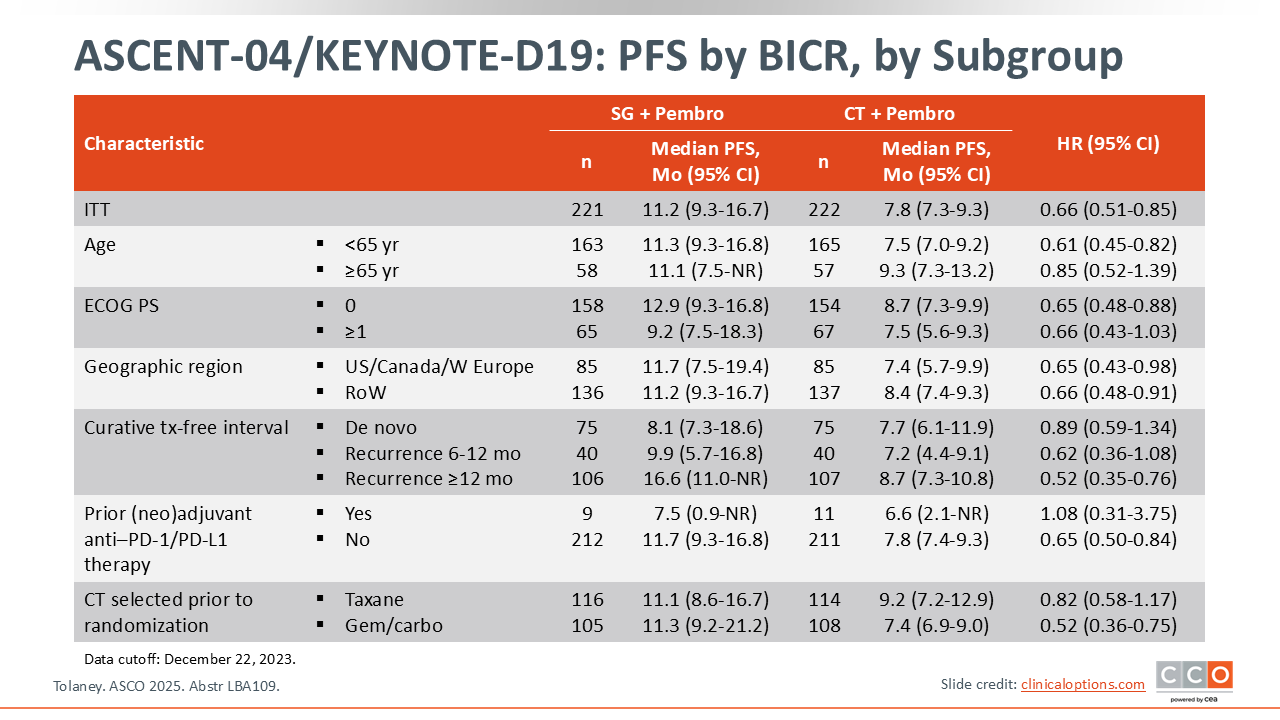
Sara M. Tolaney, MD, MPH: Looking at the subgroup analyses, the PFS benefit associated with sacituzumab govitecan plus pembrolizumab was observed across all key subgroups with the exception of those patients who had received a prior ICI in the early disease setting. It is important to be cautious when interpreting these data because there were only 20 patients who had received an ICI in the early disease setting, making the confidence intervals very large and making it difficult to draw any definitive conclusions.
ASCENT-04/KEYNOTE-D19: Response by BICR and OS
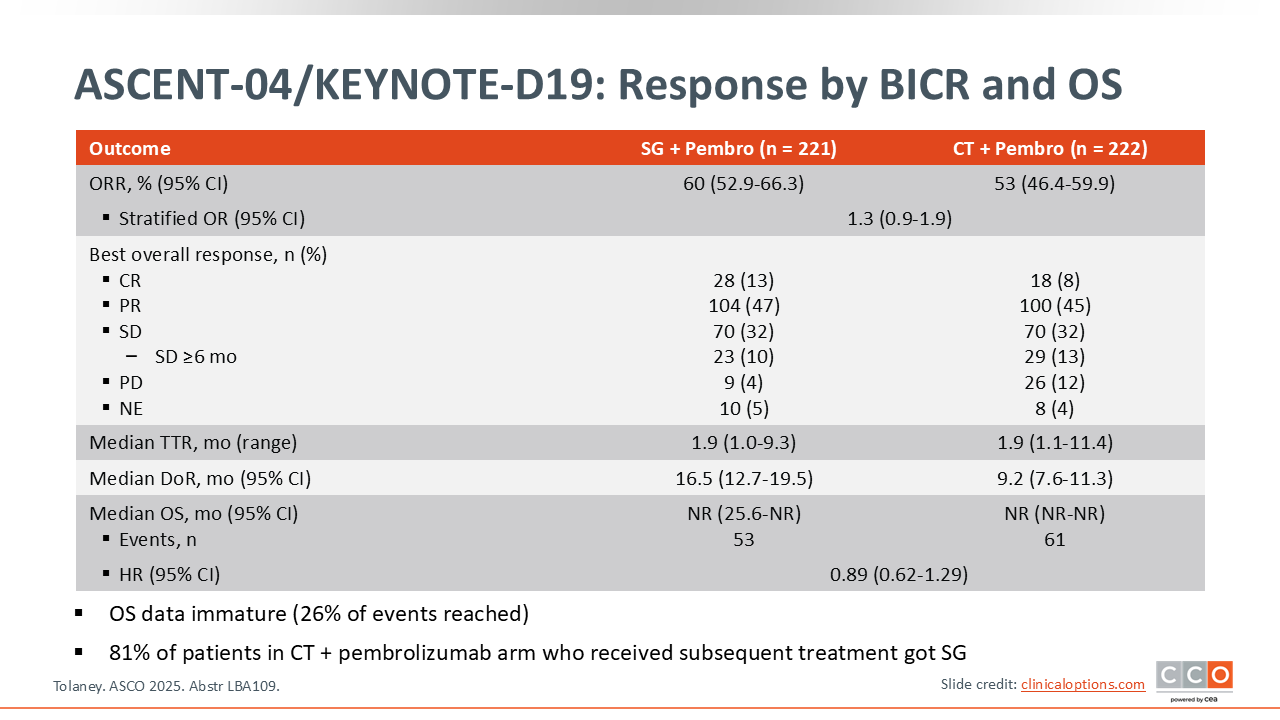
Sara M. Tolaney, MD, MPH: The ORR was numerically higher with sacituzumab govitecan plus pembrolizumab compared with chemotherapy plus pembrolizumab (60% vs 53%) and the CR rate was also numerically higher (13% vs 8% ). The OS data were very immature at this time point, but there was a trend favoring sacituzumab govitecan plus pembrolizumab with a hazard ratio of 0.89. I would note that patients who were randomized to the chemotherapy plus pembrolizumab arm were provided sacituzumab govitecan at the time of centrally confirmed disease progression, and this occurred in 81% of patients. As such, there was a very high crossover rate in this trial.
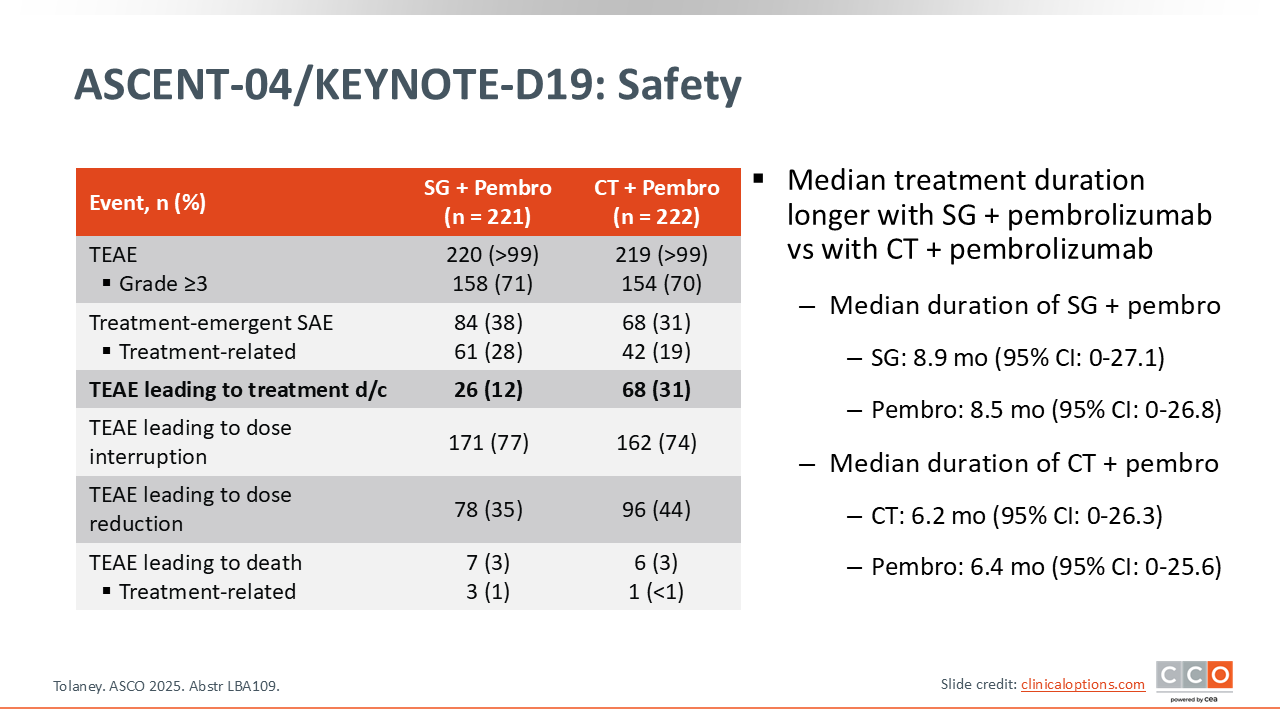
ASCENT-04/KEYNOTE-D19: Safety
Sara M. Tolaney, MD, MPH: Looking at the safety data, the number of grade 3-4 AEs was similar between the 2 arms. There were numerically more serious AEs with sacituzumab govitecan plus pembrolizumab compared with chemotherapy plus pembrolizumab, but the rate of discontinuation due to AEs was lower with sacituzumab govitecan plus pembrolizumab, with 12% of patients discontinuing sacituzumab govitecan plus pembrolizumab vs 31% with chemotherapy plus pembrolizumab.
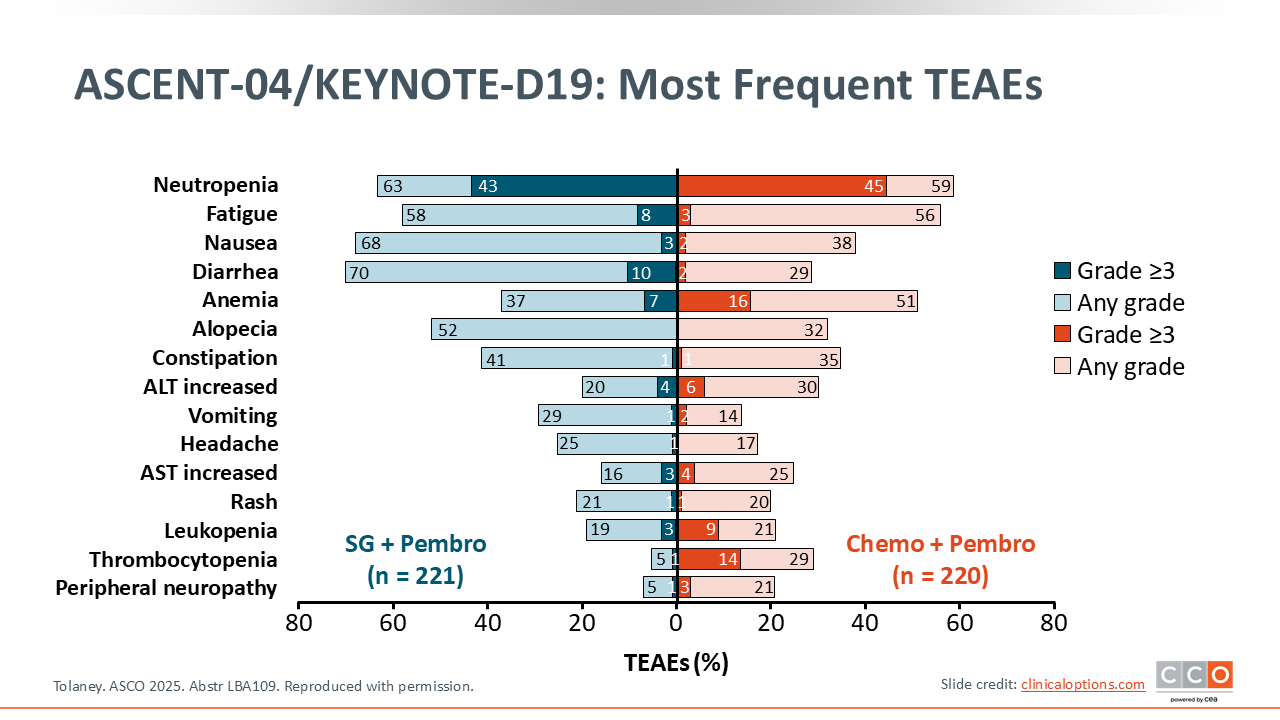
ASCENT-04/KEYNOTE-D19: Most Frequent TEAEs
Sara M. Tolaney, MD, MPH: The most common AEs observed in this trial were consistent with the toxicities known with these agents. For example, with sacituzumab govitecan plus pembrolizumab, the most common toxicities included neutropenia, fatigue, nausea, and diarrhea. With chemotherapy plus pembrolizumab neutropenia, fatigue, and anemia were common.
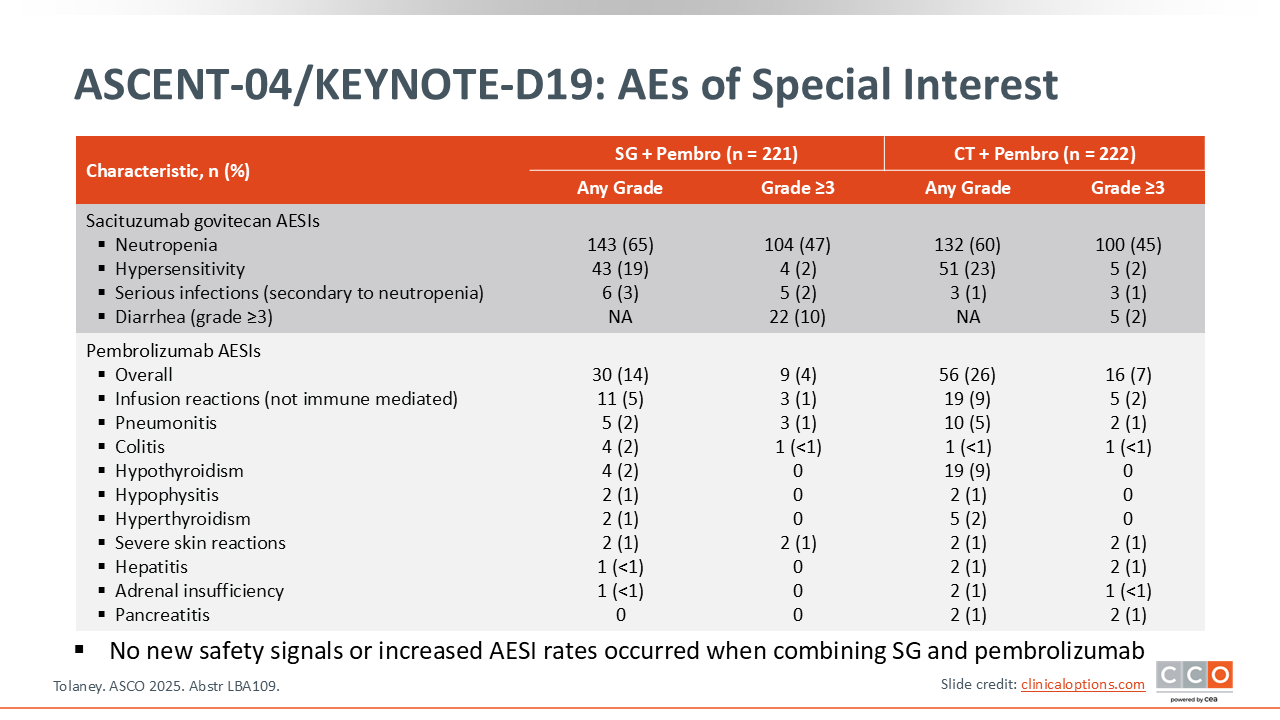
ASCENT-04/KEYNOTE-D19: AEs of Special Interest
Sara M. Tolaney, MD, MPH: One thing that we were interested in understanding with this trial was if the rate of high-grade diarrhea would increase with the addition of pembrolizumab to sacituzumab govitecan. The rate of grade 3 or higher diarrhea with sacituzumab govitecan plus pembrolizumab was 10%, which is in line with what has been observed with sacituzumab govitecan alone. This suggests that additive toxicities are not occurring. This was also true in looking at immune-related AEs, as there was no increase in the rate of these events between treatment groups.
ASCENT-04/KEYNOTE-D19: Conclusions
Sara M. Tolaney, MD, MPH: Overall, this study showed that sacituzumab govitecan plus pembrolizumab was associated with a significant improvement in PFS compared with chemotherapy plus pembrolizumab for patients with previously untreated metastatic PD-L1–positive TNBC, with a hazard ratio of 0.65. The ORR was higher and the DoR was more durable with sacituzumab govitecan plus pembrolizumab. Although survival data are still immature, there is a slight trend favoring sacituzumab govitecan plus pembrolizumab despite a very high crossover rate in this trial. Overall I think these data are very encouraging and we are certainly waiting on an approval of this combination.
Do you think that this is a regimen that we should use across the board in patients who have previously untreated metastatic PD-L1–positive TNBC?
Kevin Kalinsky, MD, MS, FASCO: I do. I think that this study was very practice-informing and compelling. I was struck by the landmark analyses, including the 12-month PFS landmark analysis where nearly 50% of patients had not had an event. Historically, we have thought of TNBC as having a median survival of approximately 12 months. I also think this study represents a moment in time, because we are going to see ADCs move into the residual disease setting. The question is how that is going to shift treatment paradigms. But for now, this study is practice-informing.
Sara M. Tolaney, MD, MPH: I agree. I think this is a tough disease and so seeing improvements is critical in that upfront setting. We also know that a lot of patients do not make it onto second-line therapy because of how aggressive this cancer is. I think it is nice to have a potential new treatment for them.
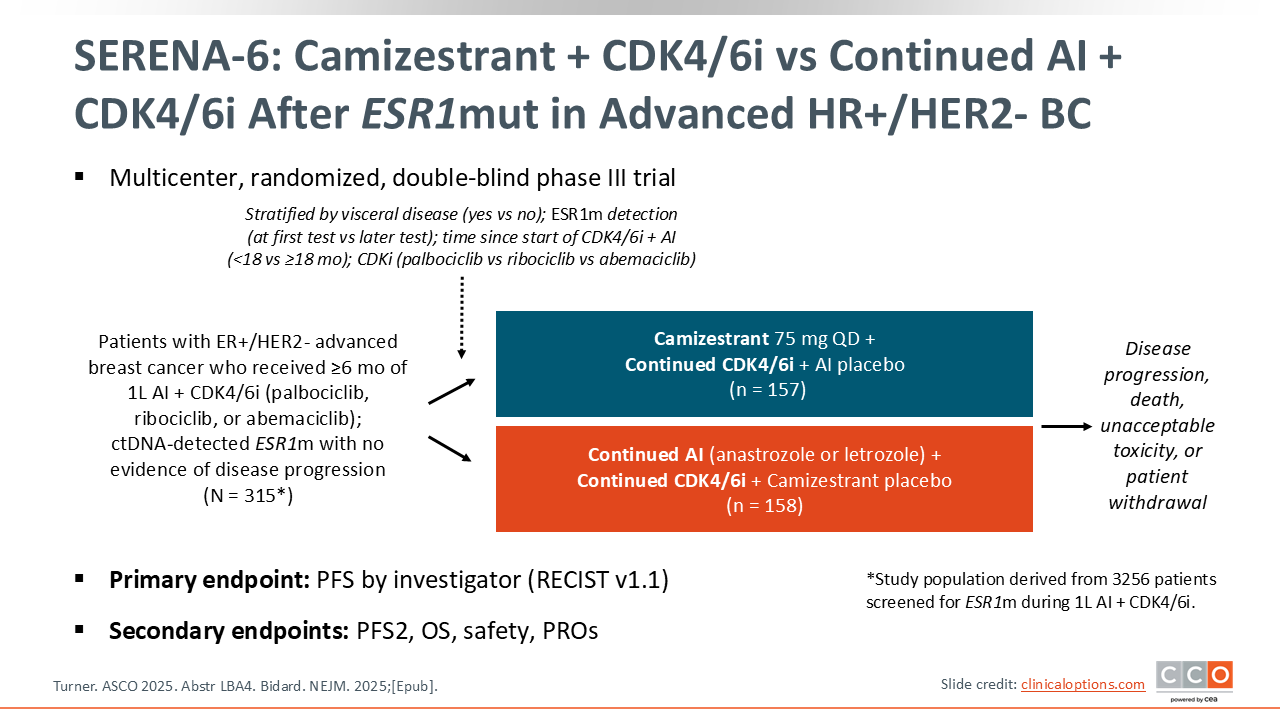
SERENA-6: Camizestrant + CDK4/6i vs Continued AI + CDK4/6i After ESR1mut in Advanced HR+/HER2- BC
Kevin Kalinsky, MD, MS, FASCO: We will now discuss the phase III SERENA-6 trial. This was a study that enrolled patients with ER-positive/HER2-negative advanced breast cancer who were receiving frontline AI and a CDK4/6 inhibitor.9,10 After 6 months, if patients had not had any radiographic progression, they could have a circulating tumor (ct)DNA evaluation. If an ESR1 mutation was detected, they were randomly assigned to receive continued treatment plus placebo or a switch to the oral selective estrogen receptor degrader (SERD) camizestrant plus continuation of their CDK4/6 inhibitor. The primary endpoint of this study was PFS by investigator.
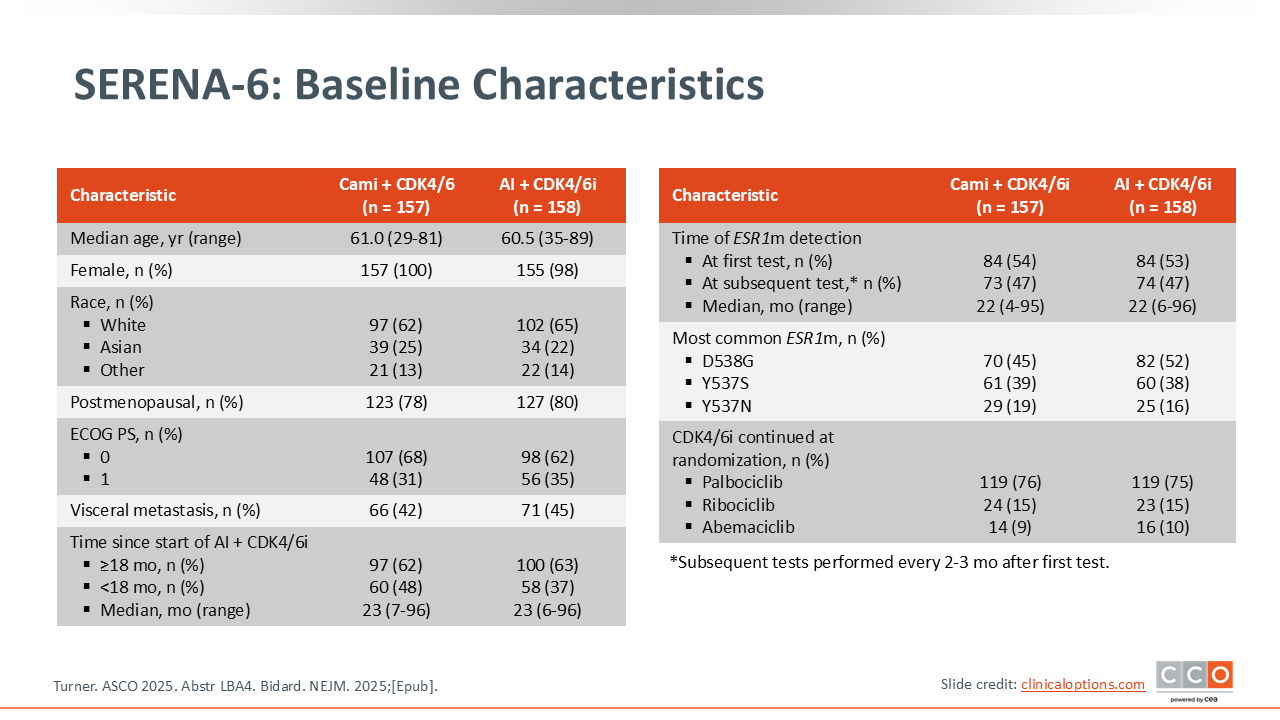
SERENA-6: Baseline Characteristics
Kevin Kalinsky, MD, MS, FASCO: Of note, the median time since the start of their AI plus CDK4/6 inhibitor was approximately 2 years. The median time of detection of an ESR1 mutation was again approximately 2 years. Approximately half of those patients had an ESR1 mutation that was detected at their first test. Also, the majority of patients were receiving palbociclib as their CDK4/6 inhibitor, with approximately 15% receiving ribociclib and approximately 10% receiving abemaciclib.
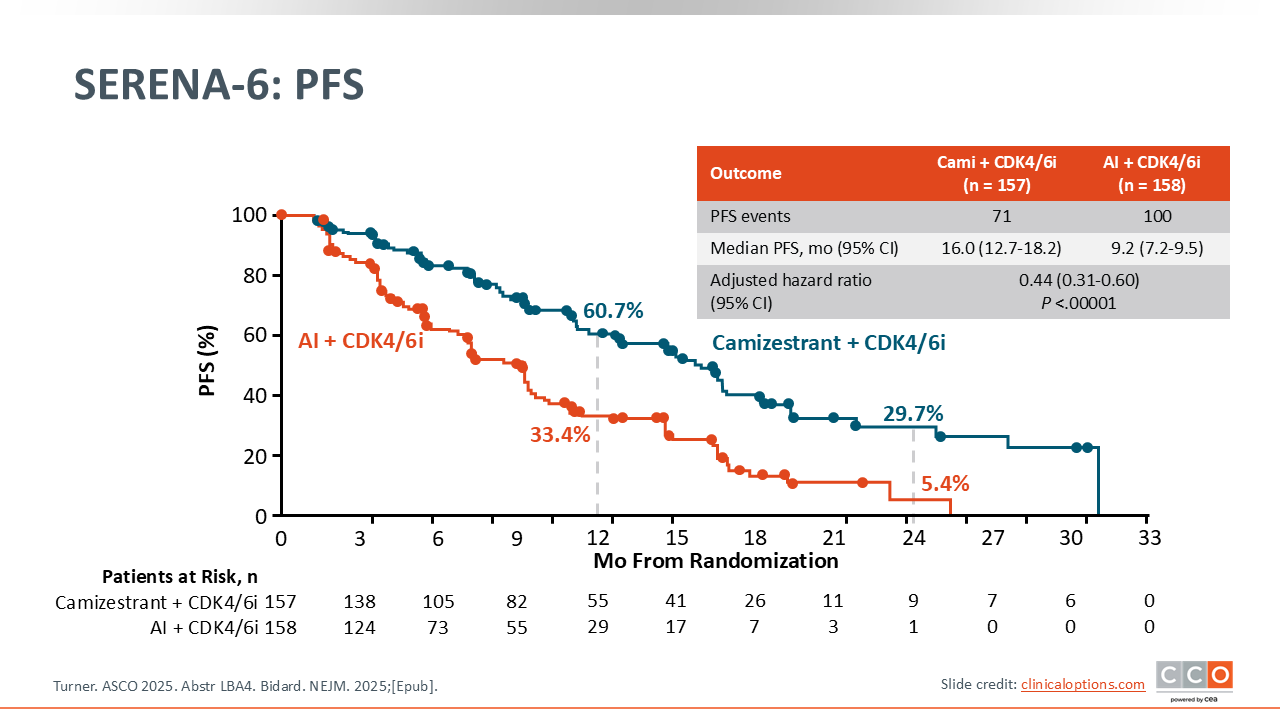
SERENA-6: PFS
Kevin Kalinsky, MD, MS, FASCO: In the camizestrant arm, there was a median PFS of 16 months vs 9.2 months with the control arm, with a hazard ratio of 0.44 and a statistically significant P value of <.00001.
Across the different subgroups that were assessed, there was not a group that did not seem to experience a PFS benefit from the switch to camizestrant.
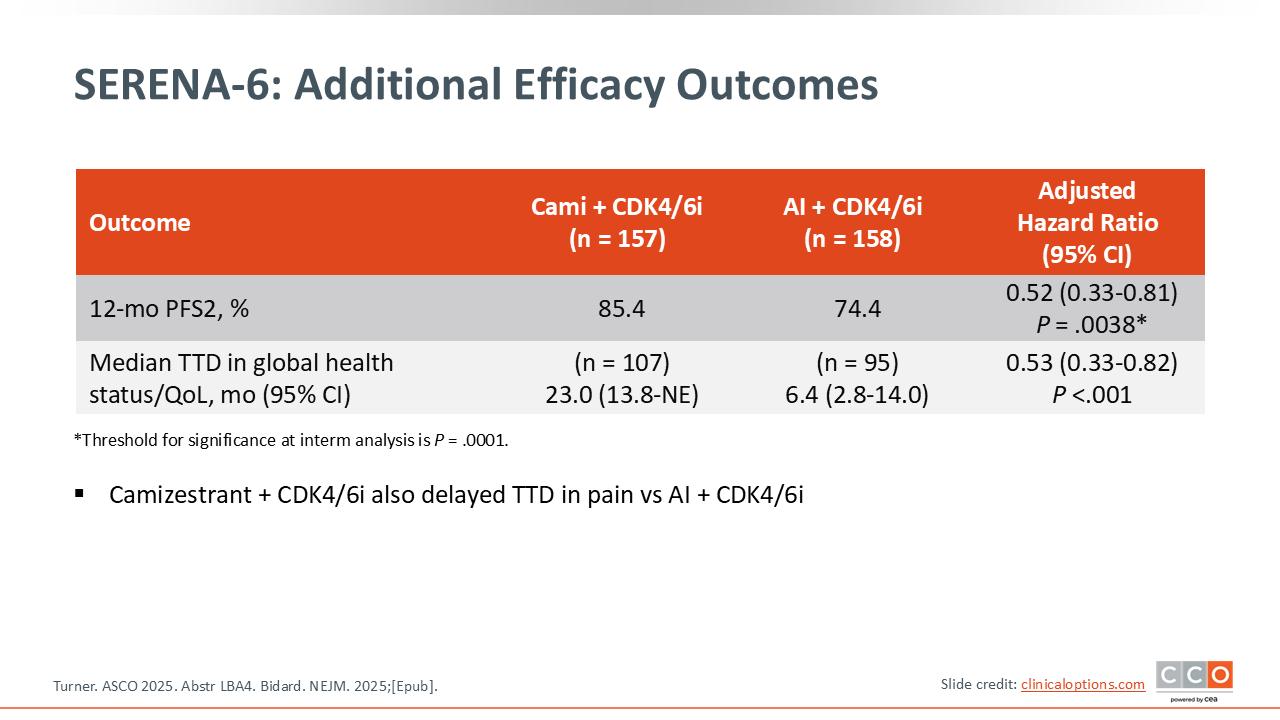
SERENA-6: Additional Efficacy Outcomes
Kevin Kalinsky, MD, MS, FASCO: Of importance, 12-month PFS2 data were available and there was a trend toward an improvement with camizestrant treatment.
The other thing that was quite interesting was that the patients who were continuing their AI had a worse GHS compared with those who received camizestrant.
SERENA-6: Most Frequent AEs
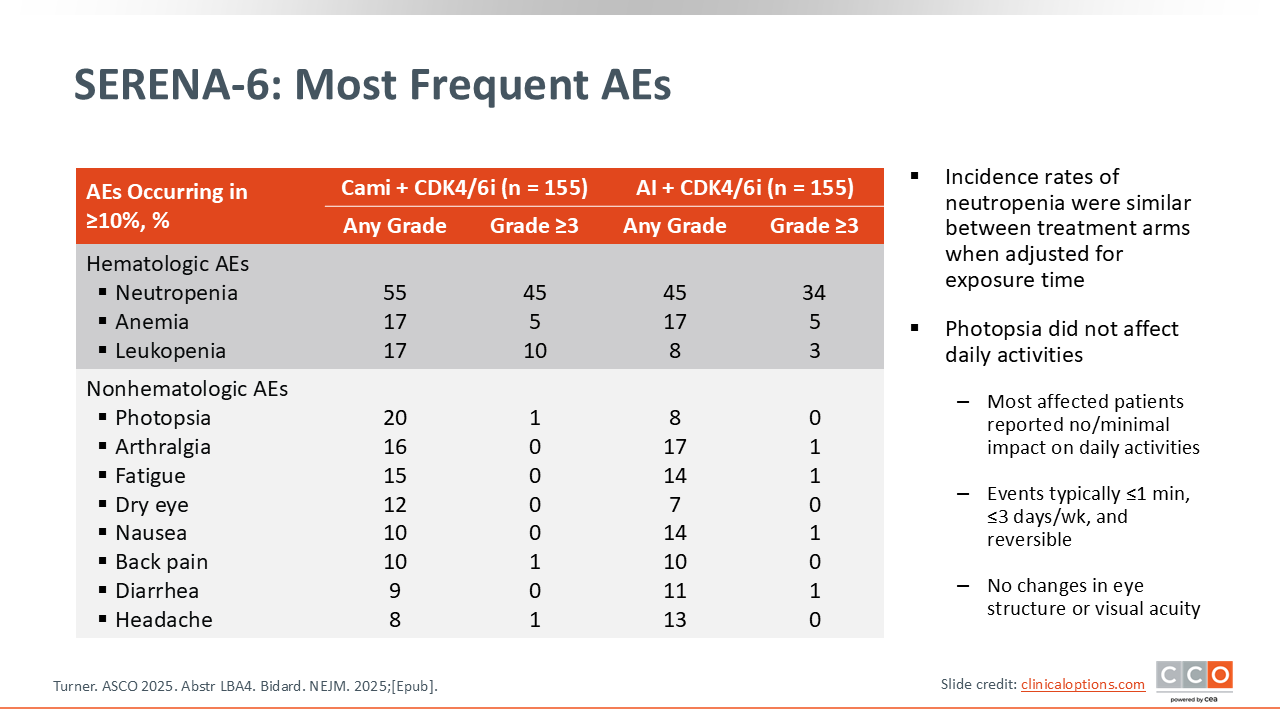
Kevin Kalinsky, MD, MS, FASCO: In terms of AEs leading to discontinuation, the rates were similar between the 2 arms.
In terms of the actual toxicities, the rate of neutropenia was similar between the 2 groups, and this was driven by the CDK4/6 inhibitor. One of the side effects associated with camizestrant in previous trials is photopsia. Photopsia has been described as your eyes taking a moment to adjust as you walk into a movie theater. In the camizestrant arm, 20% of patients experienced photopsia, but this tended to be a low-grade event.
SERENA-6: Conclusions
Kevin Kalinsky, MD, MS, FASCO: In conclusion, the SERENA-6 study did reach its primary PFS endpoint. Moving forward, it will be important to note PFS2 and OS with continued follow‑up, although there is a question as to whether this study is really powered to assess the OS endpoint.
Right now, I would say that these data are not practice-informing. Camizestrant is not an FDA-approved agent, and I would not consider the approach taken in SERENA-6 with another SERD.
Sara M. Tolaney, MD, MPH: I think this is a big paradigm shift in terms of the way we think about treating cancer, because we now generally wait until a patient experiences anatomic progression before we switch drugs. This study is asking, can we actually detect molecular resistance and then switch before anatomic progression? This was a very innovative trial. I will say I really do think this is exciting to think about.
In SERENA-6 we saw that PFS and QoL were better with a switch to camizestrant, but I think the question that we are all grappling with is whether this is going to change long-term outcomes. Will OS be different if I switch at the time of that molecular resistance mechanism rather than just waiting until anatomic progression and then putting them on a SERD, for example?
This trial makes those questions hard to really understand. I think we would have wanted to gain a better understanding of this now vs later type of question, which we cannot fully address in a trial without strict crossover. I think that is why there is a lot of trouble understanding if we should just switch over and do this for everyone.
Obviously, this trial design is super innovative and exciting. I enrolled a lot of patients onto SERENA-6 and they loved the idea of being proactive, being able to switch at the time of seeing that resistance mutation develop. I think the QoL data are actually quite provocative. I think we need to dig into this a little bit more, but patients often know when they are starting to progress. They feel it before the scan shows it, and is part of what we are seeing some of that? That patients are feeling better because they made that switch without letting their disease progress? If this really is true, it could be quite meaningful for patients to prevent all those symptoms from developing during the time of disease progression.
I think we need to understand this a little more. It will be great to see more mature PFS data from this trial, and a more detailed QoL analysis, but I think it was a really exciting study.
Kevin Kalinsky, MD, MS, FASCO: I think there are additional considerations with this type of approach, such as including the cost associated with checking ctDNA. I think the take-home is that we need more data. We need longer follow-up.
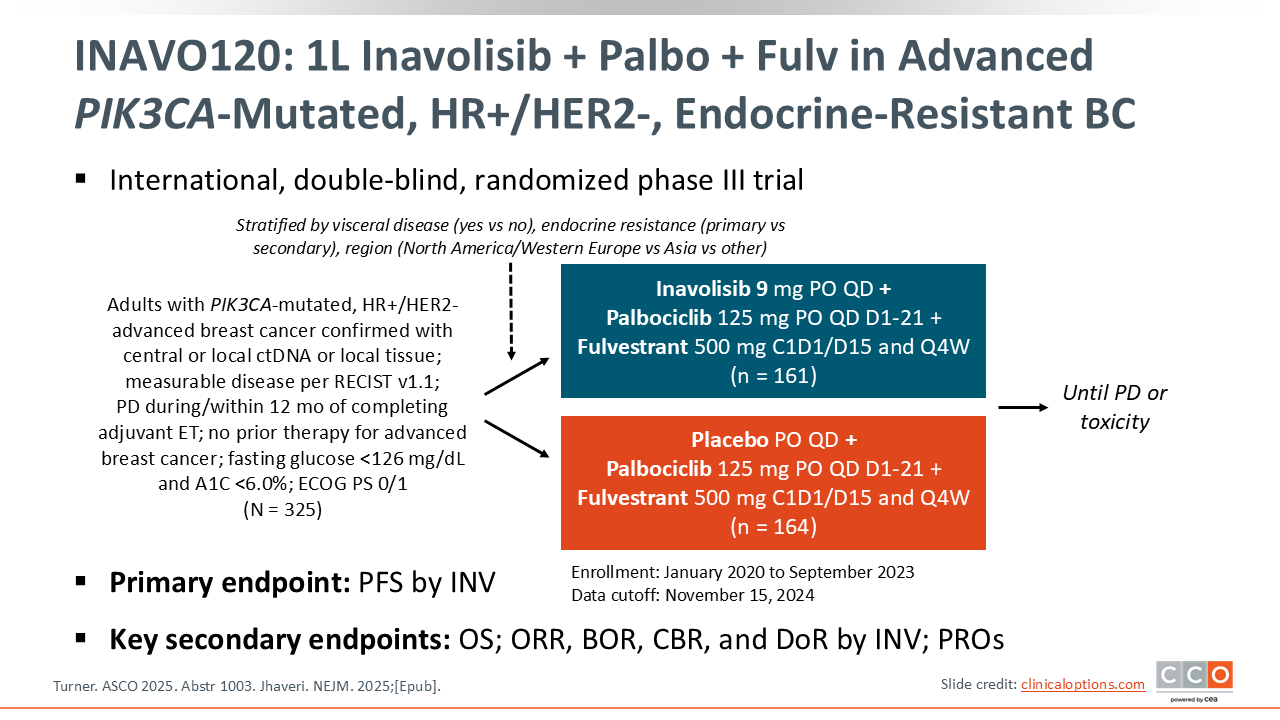
INAVO120: 1L Inavolisib + Palbo + Fulv in Advanced PIK3CA-Mutated, HR+/HER2-, Endocrine-Resistant BC
Kevin Kalinsky, MD, MS, FASCO: INAVO120 was a randomized phase III study of inavolisib or placebo plus fulvestrant and palbociclib for patients with PIK3CA-mutated, HR-positive/HER2-negative advanced breast cancer with progressive disease (PD) during or within 12 months of completing adjuvant ET and no prior therapy for advanced breast cancer.11 This was a very specific population of patients who had early recurrences, and I would also like to highlight that there was a fasting glucose requirement of less than 126 mg/dL as well as a requirement of hemoglobin A1C of less than 6%.
PFS data were previously published for this study, demonstrating significantly improved median PFS with inavolisib vs placebo (15.0 vs 7.3 months; HR: 0.43; P <.001). This led to the FDA approval of inavolisib in combination with palbociclib and fulvestrant for the treatment of adults with endocrine-resistant, PIK3CA-mutated, HR-positive, HER2-negative, locally advanced or mBC following recurrence on or after completing adjuvant ET.
At ASCO 2025, OS data and updated PFS data were presented.12,13
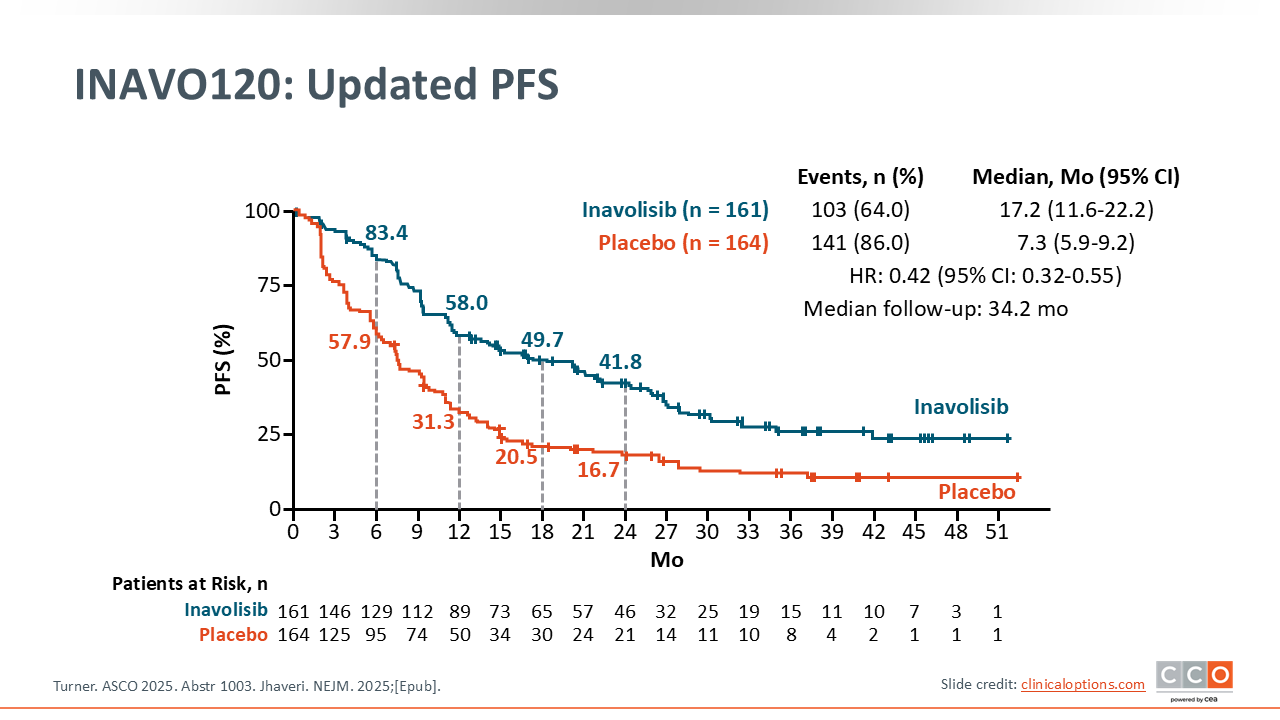
INAVO120: Updated PFS
Kevin Kalinsky, MD, MS, FASCO: The data with updated PFS were quite impressive. An almost 10-month improvement in median PFS was observed with inavolisib vs placebo (17.2 vs 7.3 months; HR: 0.42), now with a median follow-up of 34.2 months. In looking at the slopes of the PFS curves, it is clear from the placebo arm how poorly patients with this type of tumor do, and what an improvement in outcomes they can have with the addition of inavolisib.
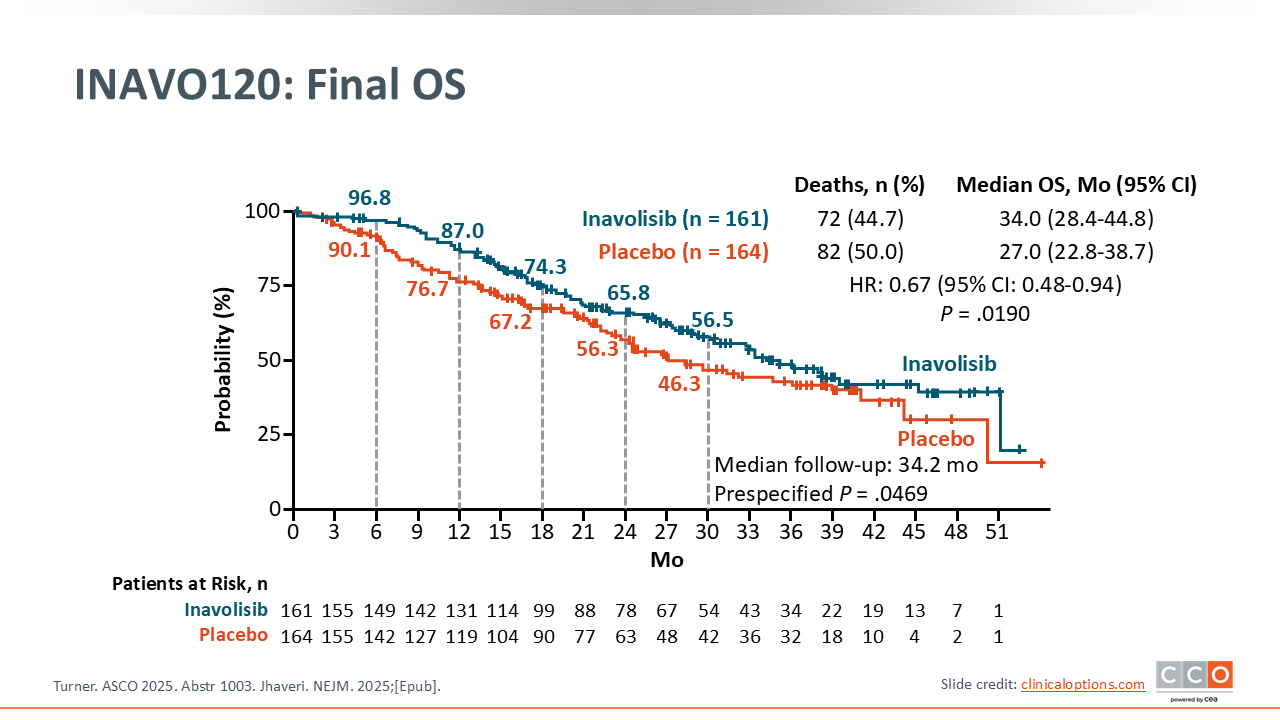
INAVO120: Final OS
Kevin Kalinsky, MD, MS, FASCO: We also saw an improvement in median OS of approximately 7 months with inavolisib vs placebo (34.0 vs 27.0 months; HR: 0.67; P = .019). This study did not allow crossover.
In looking at the OS by subgroup, all populations appeared to benefit with the addition of inavolisib.
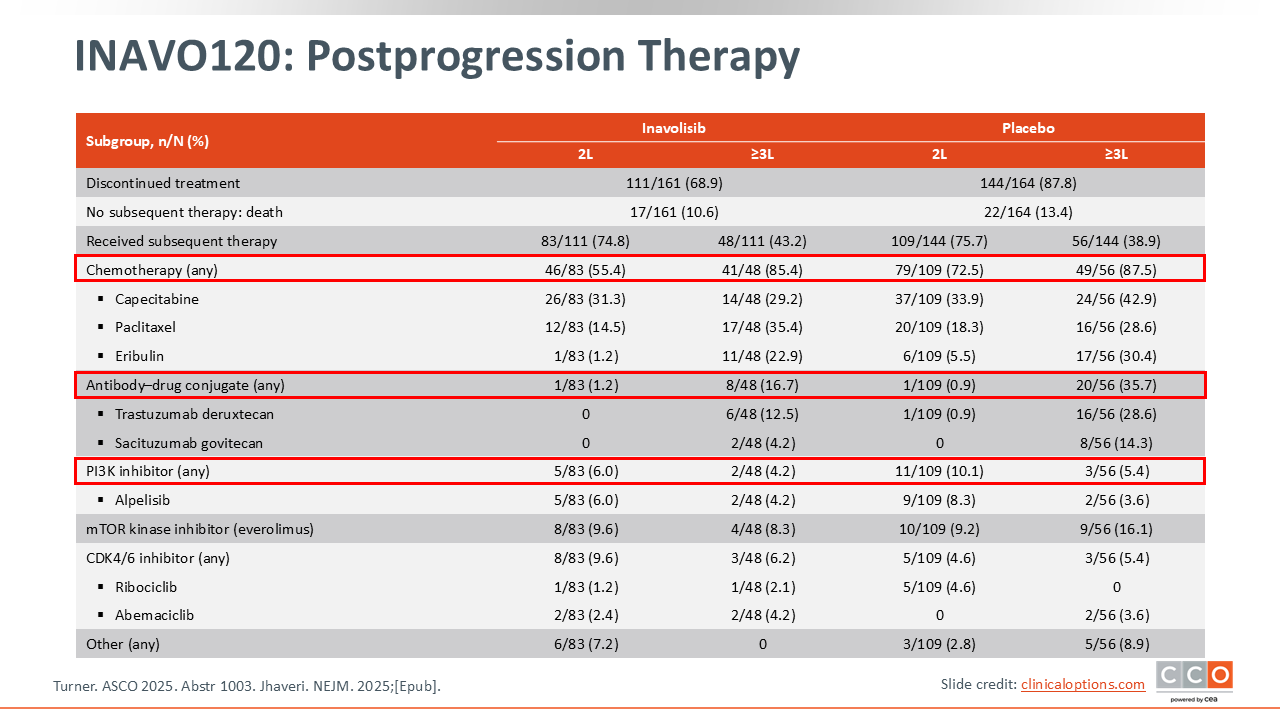
INAVO120: Postprogression Therapy
Kevin Kalinsky, MD, MS, FASCO: In terms of what patients received after progression, following inavolisib-based therapy, approximately 50% of patients received chemotherapy, few received an ADC, and approximately 6% received a PI3K inhibitor. Of note, in the placebo arm in the second-line setting, approximately three quarters of patients received chemotherapy, with very few receiving an ADC or PI3K inhibitor.
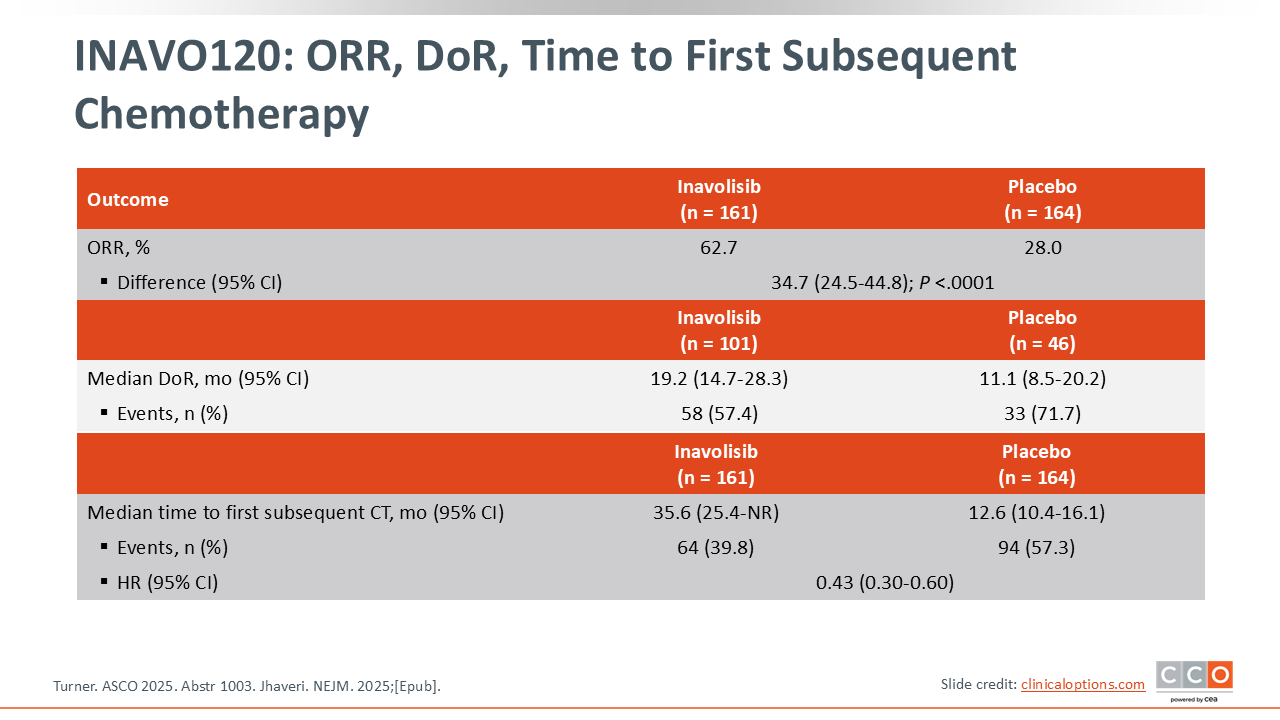
INAVO120: ORR, DoR, Time to First Subsequent Chemotherapy
Kevin Kalinsky, MD, MS, FASCO: It was also notable that patients receiving inavolisib had a longer median time to subsequent chemotherapy compared with those in the placebo arm (35.6 vs 12.5 months).
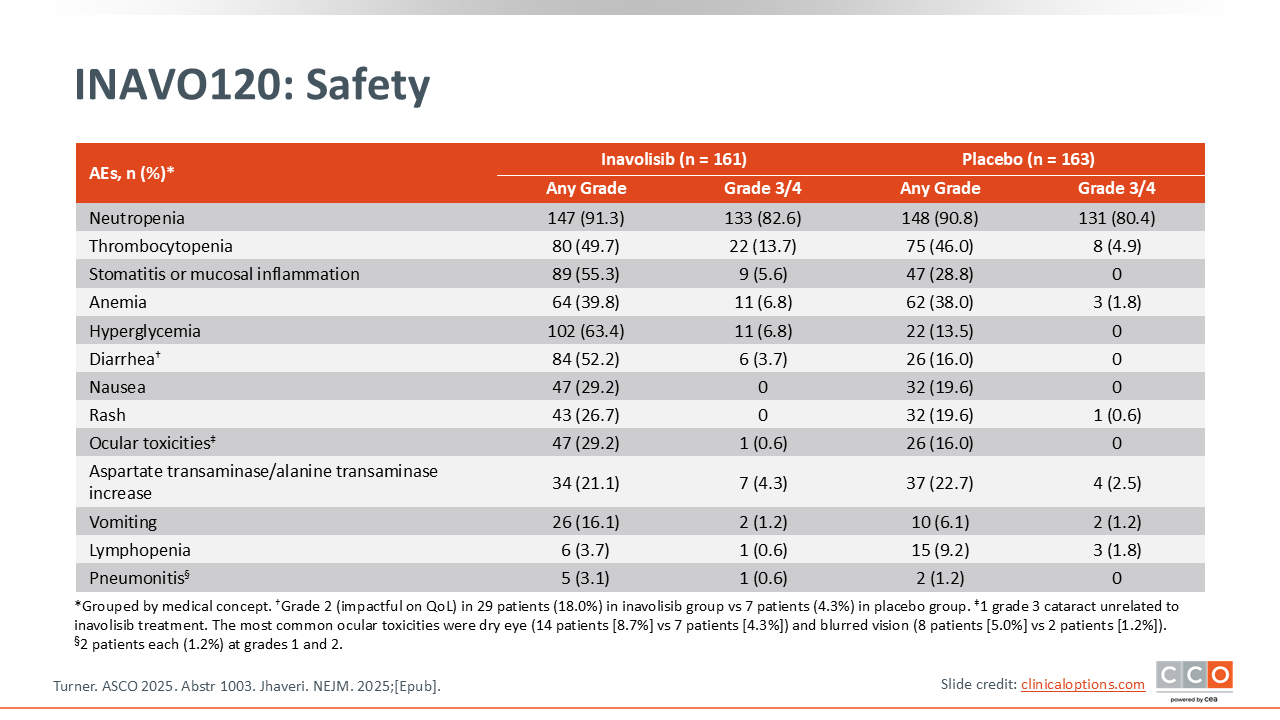
INAVO120: Safety
Kevin Kalinsky, MD, MS, FASCO: Safety had been previously described. I would like to highlight key side effects when adding inavolisib to palbociclib. One of the things to really look out for with this regimen beyond hyperglycemia is stomatitis. I have found that it can be helpful to use a steroid rinse preventatively for this AE.
INAVO120: Conclusions
Kevin Kalinsky, MD, MS, FASCO: Ultimately, we saw an improvement in PFS and OS with the addition of inavolisib to fulvestrant and palbociclib for patients with PIK3CA-mutated, HR-positive/HER2-negative advanced breast cancer with PD during or within 12 months of completing adjuvant ET and no prior therapy for advanced breast cancer. It is worth mentioning that this is the first time we have seen an OS improvement with a PI3K/AKT pathway inhibitor. In my practice, I considered INAVO120 a practice-informing study prior to this presentation, but I do think that these data further reinforced for this population that we should consider utilizing a triplet.
Sara M. Tolaney, MD, MPH: I agree, I had already changed practice before seeing the mature OS data because the PFS data were striking. To see such a large difference—more than a doubling of PFS—is a big deal. These were patients who recurred on or within a year of adjuvant ET. They were patients whose disease was endocrine-refractory and had a PI3K mutation. Patients in the control arm did not do very well and there was a tremendous benefit from adding the PI3K inhibitor. I think it is a really important strategy to screen our patients in the first-line setting to know there is a PI3K mutation upfront.
One of the limitations of this study, however, is that it was conducted at a time when patients had not received an adjuvant CDK4/6 inhibitor. In the current era, as we may start seeing patients recur after adjuvant CDK4/6 inhibitor treatment, the question will arise as to how effective the INAVO120 strategy will be in a patient who has received a CDK4/6 inhibitor before. We just do not have data on that scenario at this time, and so that does remain an open question.
Kevin Kalinsky, MD, MS, FASCO: We are now increasingly evaluating PI3K mutation–specific inhibitors, and the field is evolving in terms of the agents that we have at our disposal.
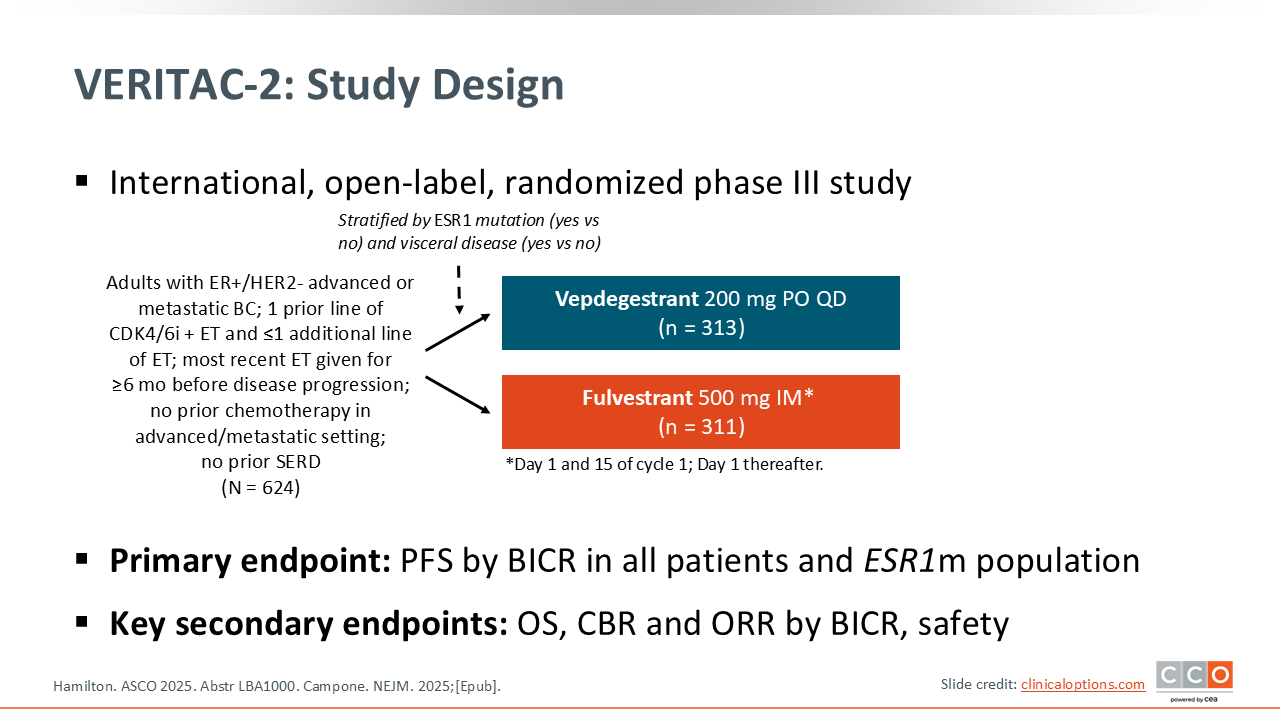
VERITAC-2: Study Design
Kevin Kalinsky, MD, MS, FASCO: We will also briefly touch on a few additional studies in advanced breast cancer. VERITAC-2 was a phase III study that enrolled patients with ER-positive/HER2-negative advanced or mBC with 1 prior line of CDK4/6 inhibitor + ET and ≤1 additional line of ET with no prior chemotherapy in the advanced/metastatic setting and no prior SERD.14,15 Patients were randomized to vepdegestrant (an oral PROTAC ER degrader targeting wild-type and mutant ER) or fulvestrant, with the primary endpoint of PFS by BICR in all patients and ESR1-mutant population.
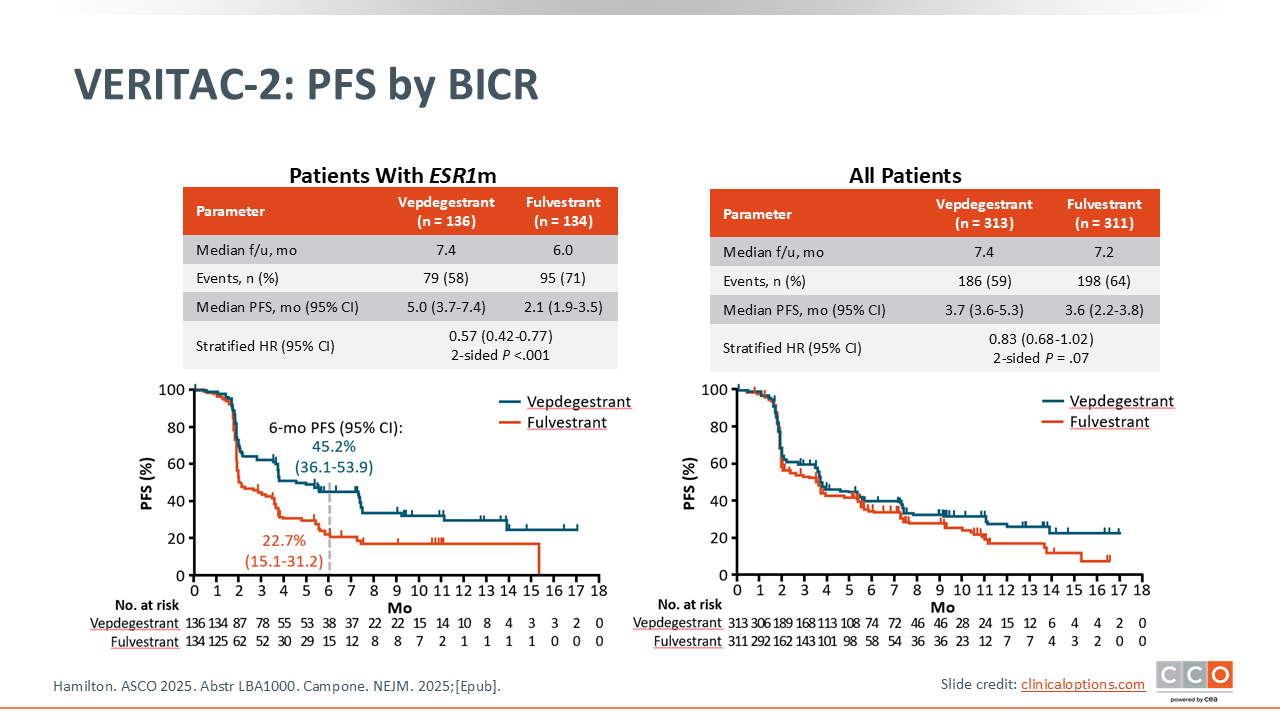
VERITAC-2: PFS
Kevin Kalinsky, MD, MS, FASCO: In patients with ESR1-mutant disease, vepdegestrant was associated with a median PFS of 5.0 months vs 2.1 months with fulvestrant (HR: 0.57; P <.001). Of note, this difference was not observed in the overall population (median PFS: 3.7 vs 3.6 months; HR: 0.83; P = .7). The investigators concluded that vepdegestrant is a potential new oral therapy option for patients with previously treated ESR1-mutant ER-positive/HER2-negative advanced breast cancer.
Based on these data, vepdegestrant could be a good option for patients similar to those in VERITAC-2 if approved. This therapeutic is well tolerated, and I would likely give as a single agent.
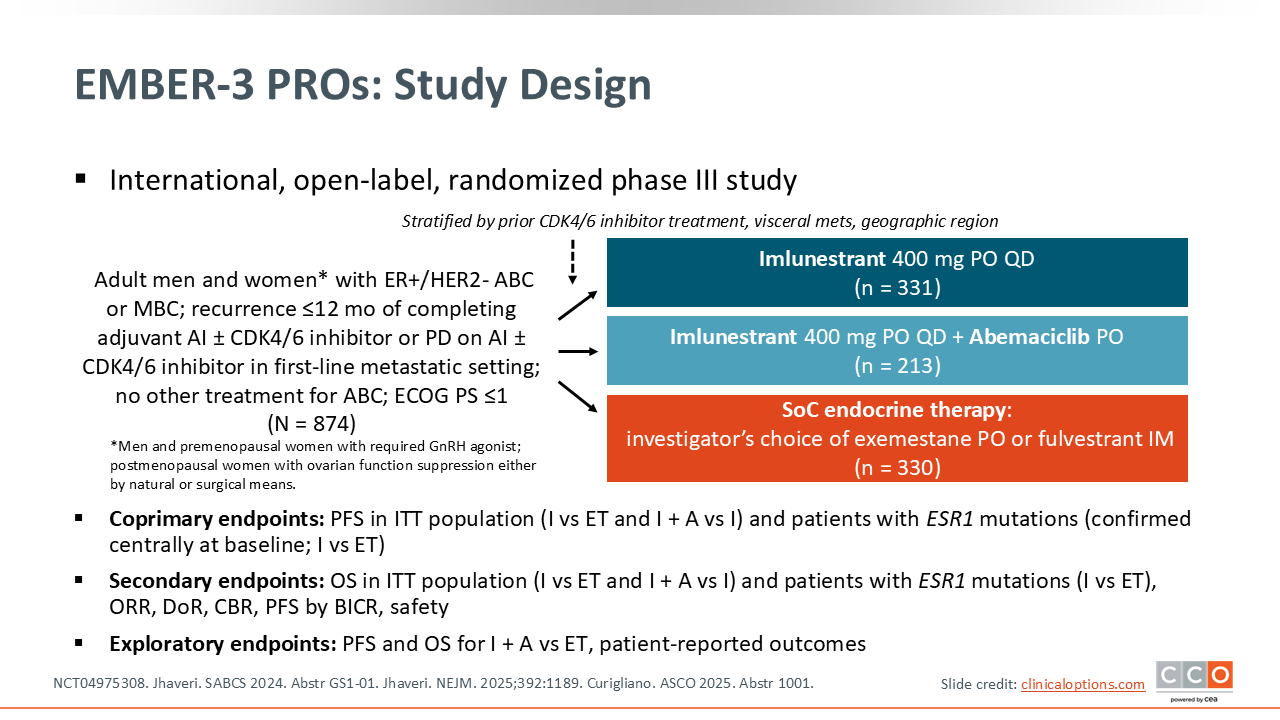
EMBER-3: PROs: Study Design
Sara M. Tolaney, MD, MPH: EMBER-3 was a phase III study that evaluated imlunestrant, an oral SERD, with or without abemaciclib vs SoC ET in patients with advanced ER-positive/HER2-negative breast cancer and disease progression on or following AI ± CDK4/6 inhibitor therapy.16 The primary analysis of this study was previously reported, demonstrating:
The current report explored patient-reported outcomes among participants in EMBER-3.17
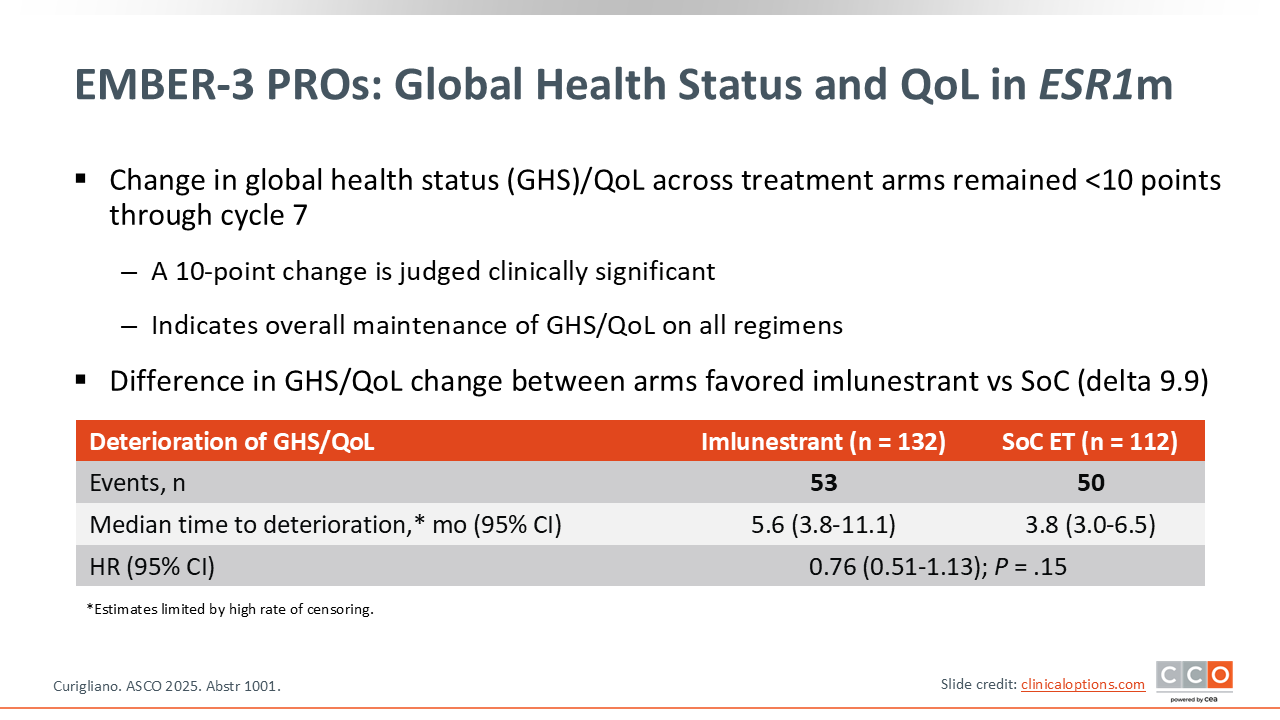
EMBER-3 PROs: Global Health Status and QoL With ESR1m
Sara M. Tolaney, MD, MPH: In patients with ESR1-mutated disease, longitudinal difference in GHS/QoL and time to deterioration of GHS/QoL numerically favored imlunestrant vs SoC ET (time to deterioration: 5.6 vs 3.8 months; HR: 0.76; P = .15)
Patient-reported GHS/QoL and functional domains remained stable irrespective of treatment arm. Most symptom domains remained stable in all treatment arms, other than an anticipated increase in diarrhea, nausea, and vomiting with use of imlunestrant with abemaciclib. The rate of reported frequent or almost constant diarrhea was higher with imlunestrant plus abemaciclib compared with imlunestrant or SoC ET (22% vs 3% vs 2%, respectively).
The investigators concluded that the current analysis supports the overall findings of EMBER-3 regarding benefit associated with imlunestrant with or without abemaciclib as a targeted therapy option for patients with ER-positive/HER2-negative advanced breast cancer and PD on ET.
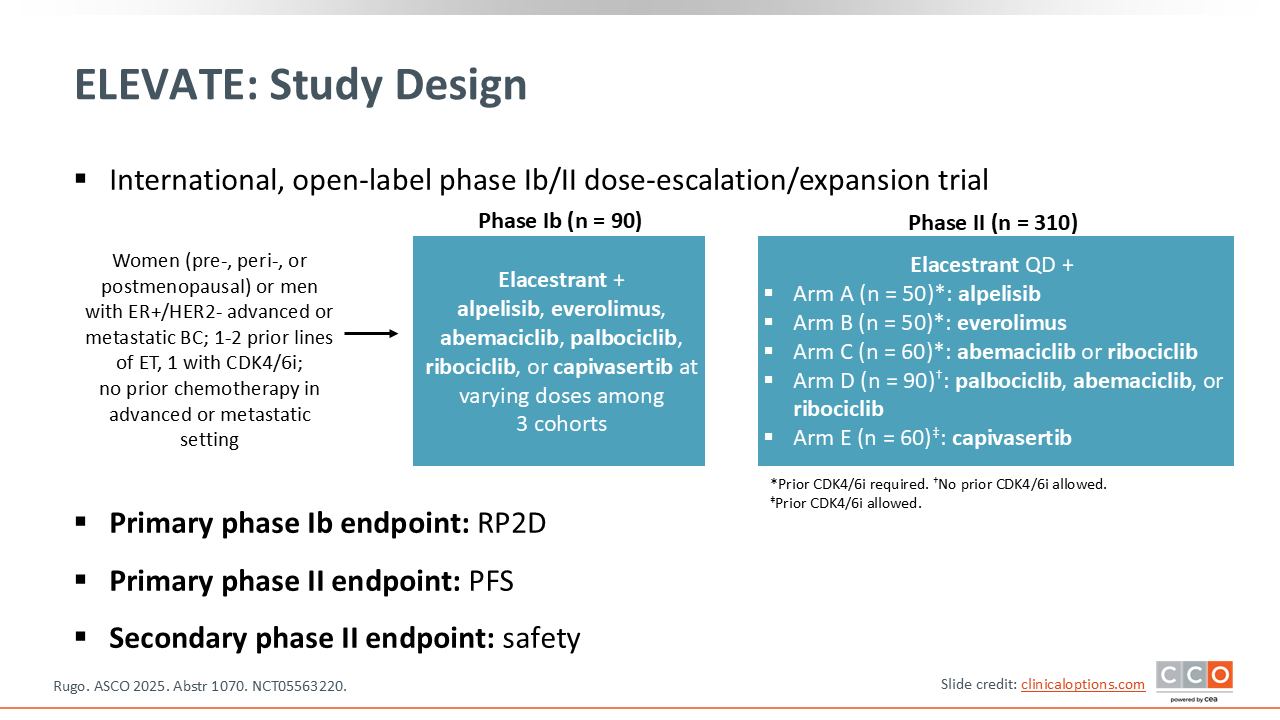
ELEVATE: Study Design
Sara M. Tolaney, MD, MPH: Elacestrant is the first FDA-approved oral SERD indicated for treating patients with ER-positive, HER2-negative, ESR1-mutated advanced or mBC with disease progression following 1 or more line of ET (based on improved mPFS in the phase III EMERALD study).18
ELEVATE is an open-label phase Ib/II dose-escalation/expansion trial assessing elacestrant plus everolimus, ribociclib, and additional combinations in patients with ER-positive/HER2-negative locally advanced or mBC with 1-2 prior lines of ET (1 with a CDK4/6 inhibitor) and no prior chemotherapy in the advanced or metastatic setting.19 At ASCO 2025, updated safety and efficacy data were presented from the elacestrant plus everolimus or ribociclib cohorts of this trial.
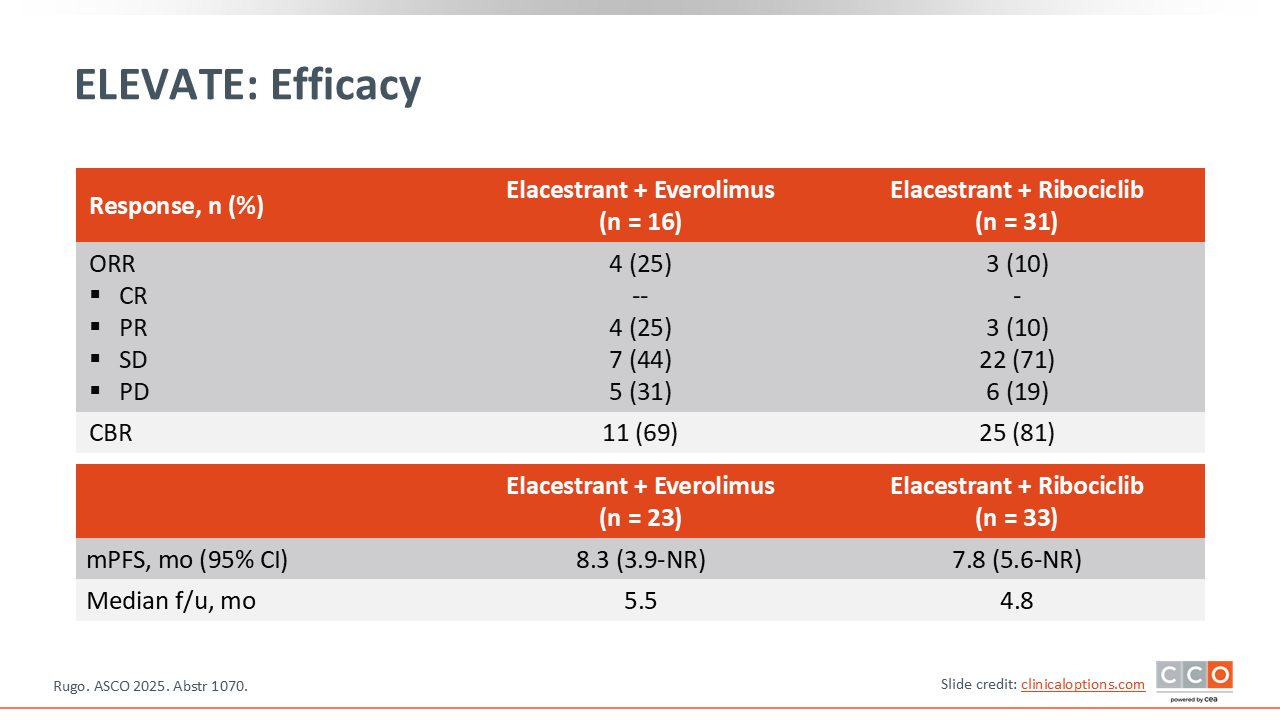
ELEVATE: Efficacy
Sara M. Tolaney, MD, MPH: Clinically meaningful efficacy was observed with elacestrant combinations, regardless of ESR1 mutation status (median PFS: elacestrant plus everolimus, 8.3 months; elacestrant plus ribociclib, 7.8 months).
Elacestrant combinations also demonstrated safety profiles consistent with established combinations of ET with ribociclib or everolimus.
Investigators concluded that elacestrant has the potential to serve as an ET backbone for a range of targeted agents, providing an all-oral treatment option for patients with ER-positive/HER2-negative mBC and potentially delaying the need for chemotherapy or ADC-based therapies.
neoCARHP: Study Design
Sara M. Tolaney, MD, MPH: Let us now review some key findings from studies of novel treatment strategies for EBC.
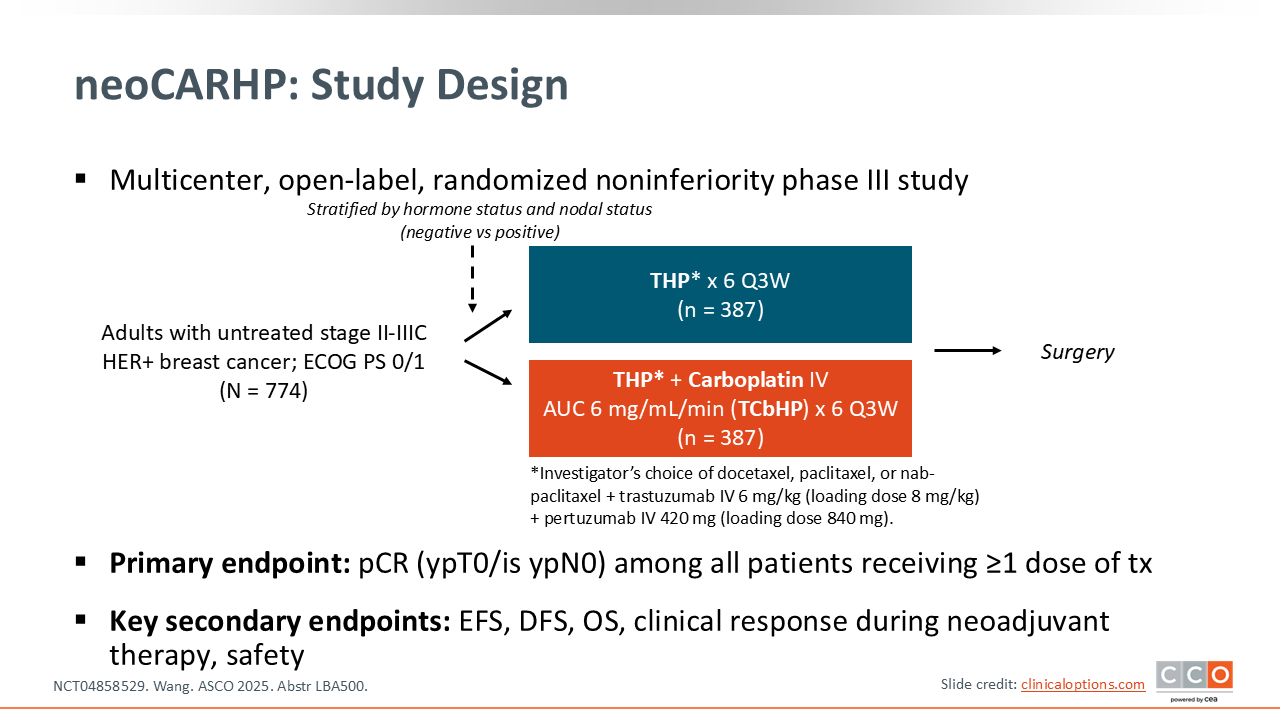
neoCARHP was a randomized phase III study of de-escalated neoadjuvant taxane plus trastuzumab and pertuzumab with or without carboplatin in patients with untreated stage II-IIIC HER2-positive breast cancer.20 The primary endpoint was pathologic complete response (pCR) (ypT0/is ypN0) among all patients receiving 1 or more dose of treatment.
neoCARHP: pCR (Primary Endpoint) and Clinical Response
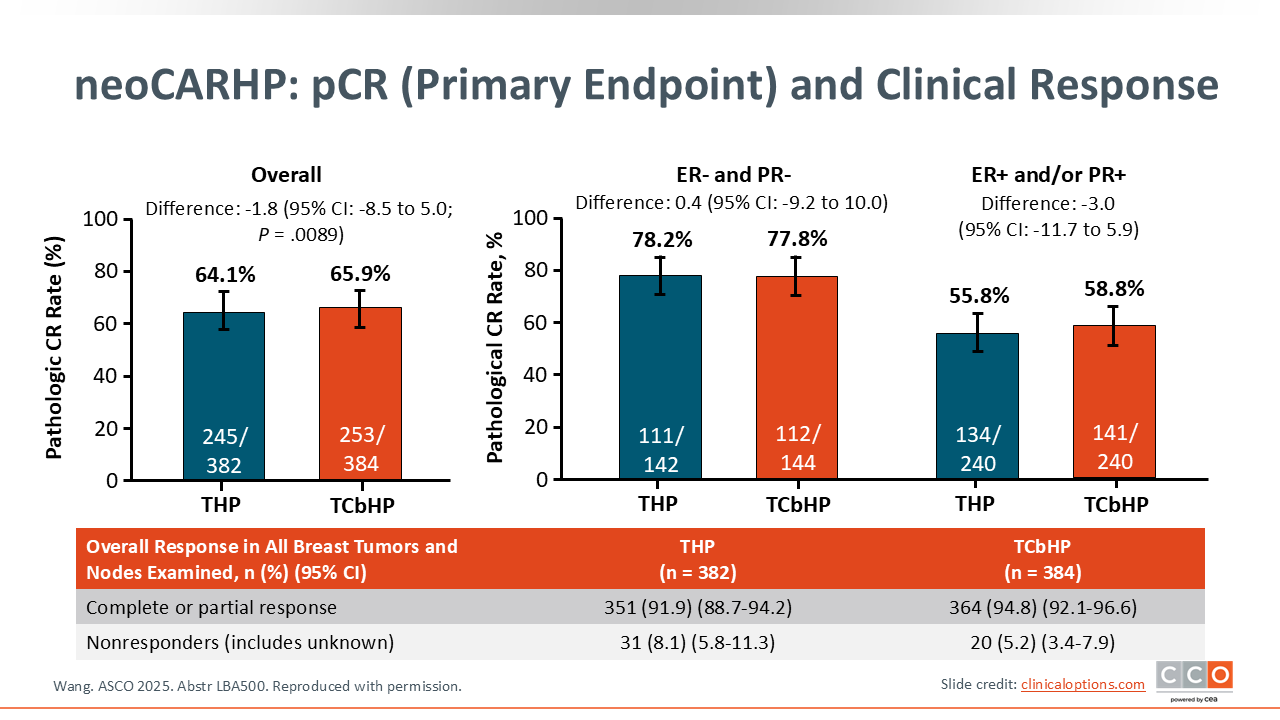
Sara M. Tolaney, MD, MPH: THP was noninferior to TCbHP as measured by pCR (64.1% vs 65.9% (P = .0089). Clinical response during neoadjuvant therapy was also comparable (91.9% vs 94.8%).
Improved tolerability was observed with THP based on fewer grade 3/4 AEs. The investigators concluded that omission of carboplatin with dual HER2 blockade could be a valuable de-escalated neoadjuvant strategy for patients with HER2-positive EBC while maintaining an every-3-week dosing schedule.
NATALEE: Study Design
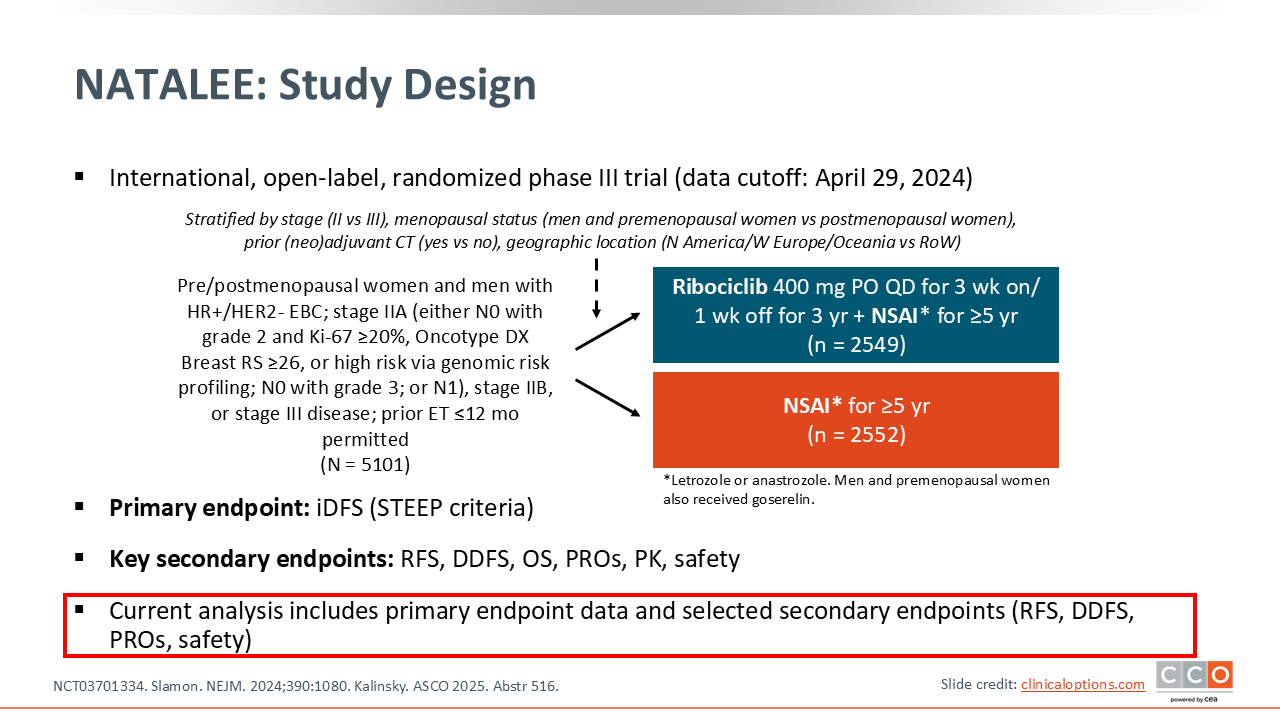
Kevin Kalinsky, MD, MS, FASCO: NATALEE was a randomized phase III trial comparing the addition of ribociclib to adjuvant ET with a NSAI vs an NSAI alone in patients with intermediate- to high‑risk HR-positive/HER2-negative EBC.21
The primary endpoint was iDFS. The interim analysis of iDFS, which was published in 2024, reported that adding ribociclib to adjuvant NSAI therapy significantly improved iDFS vs an NSAI alone. The final iDFS analysis confirmed the findings of the interim analysis.22 For the 3-year iDFS analysis, investigators reported an iDFS rate of 90.7% with adjuvant ribociclib plus an NSAI vs 87.6% with an NSAI alone, yielding an absolute difference of 3.1% in favor of ribociclib. Adding ribociclib to adjuvant NSAI therapy significantly reduced the risk of invasive disease by 25.1% vs treatment with an NSAI alone (HR: 0.749; P = .0012).
At ASCO 2025, an analysis from the NATALEE trial reported 4-year efficacy, safety, and QoL data for ribociclib plus an NSAI vs an NSAI alone by age and menopausal status.23
NATALEE: iDFS by Menopausal Status
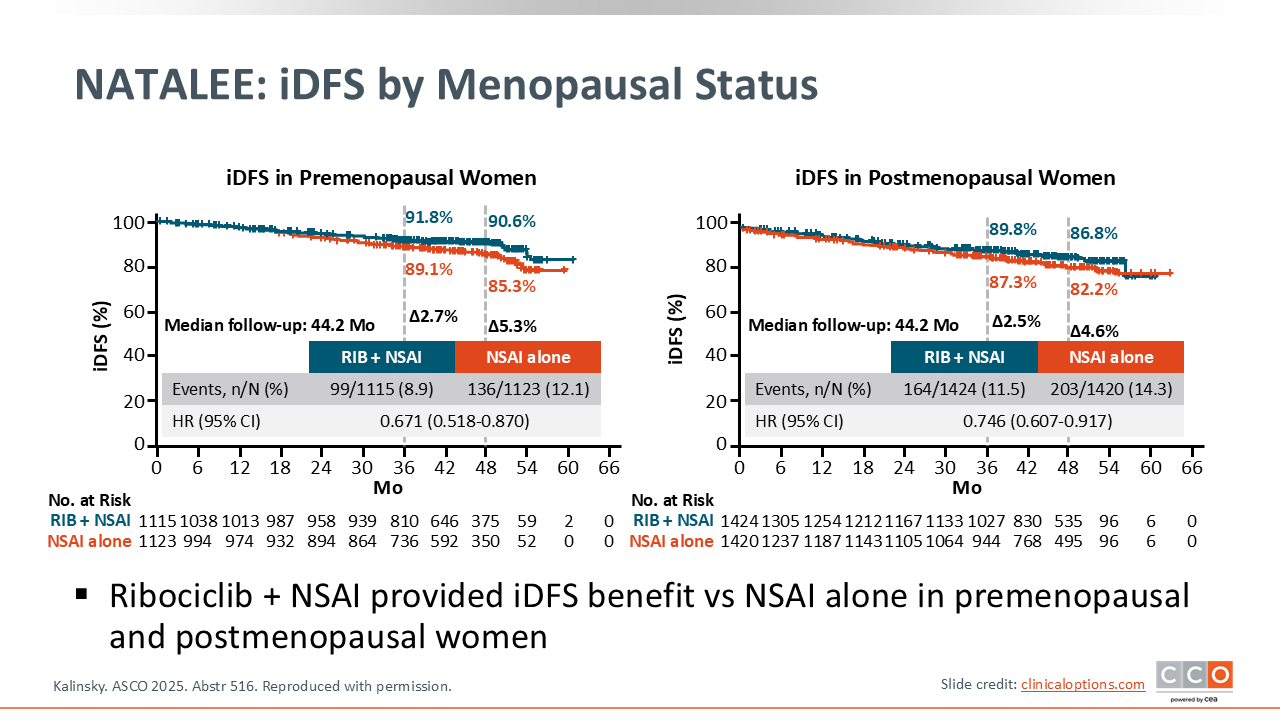
Kevin Kalinsky, MD, MS, FASCO: Data presented at ASCO 2025 showed that ribociclib plus an NSAI provided an iDFS benefit compared to an NSAI alone in premenopausal (48-month: 90.6% vs 85.3%; Δ 5.3%; HR: 0.671) and postmenopausal women (48-month: 86.8% vs 82.2%; Δ 4.6%; HR: 0.746) with intermediate- to high‑risk HR-positive/HER2-negative EBC.
Investigators concluded that ribociclib plus an NSAI provides clinical benefit to a broad population of patients with stage II/III HR-positive/HER2-negative EBC.
Let’s return to our questions from earlier.