CE / CME
Physician Assistants/Physician Associates: 0.75 AAPA Category 1 CME credit
ABIM MOC: maximum of 0.75 Medical Knowledge MOC point
Nurse Practitioners/Nurses: 0.75 Nursing contact hour
Physicians: maximum of 0.75 AMA PRA Category 1 Credit™
Released: March 27, 2025
Expiration: March 26, 2026
Reasons for Seeking Early Diagnosis
Sharon Cohen, MD, FRCPC:
I am a behavioral neurologist located in Toronto, Canada. I am a practicing HCP working in the trenches, seeing people with memory concerns and other cognitive problems. I am also a clinical trialist, very much interested in moving the needle on new treatments for Alzheimer's disease (AD) and related disorders.
Preventing brain disease is important. The brain is precious and wonderful. We often take for granted that we can think, speak, reflect on things, move, and sense things until we lose those abilities. I feel my work must move towards prevention, ensuring that we do not let people become disabled by brain disease.
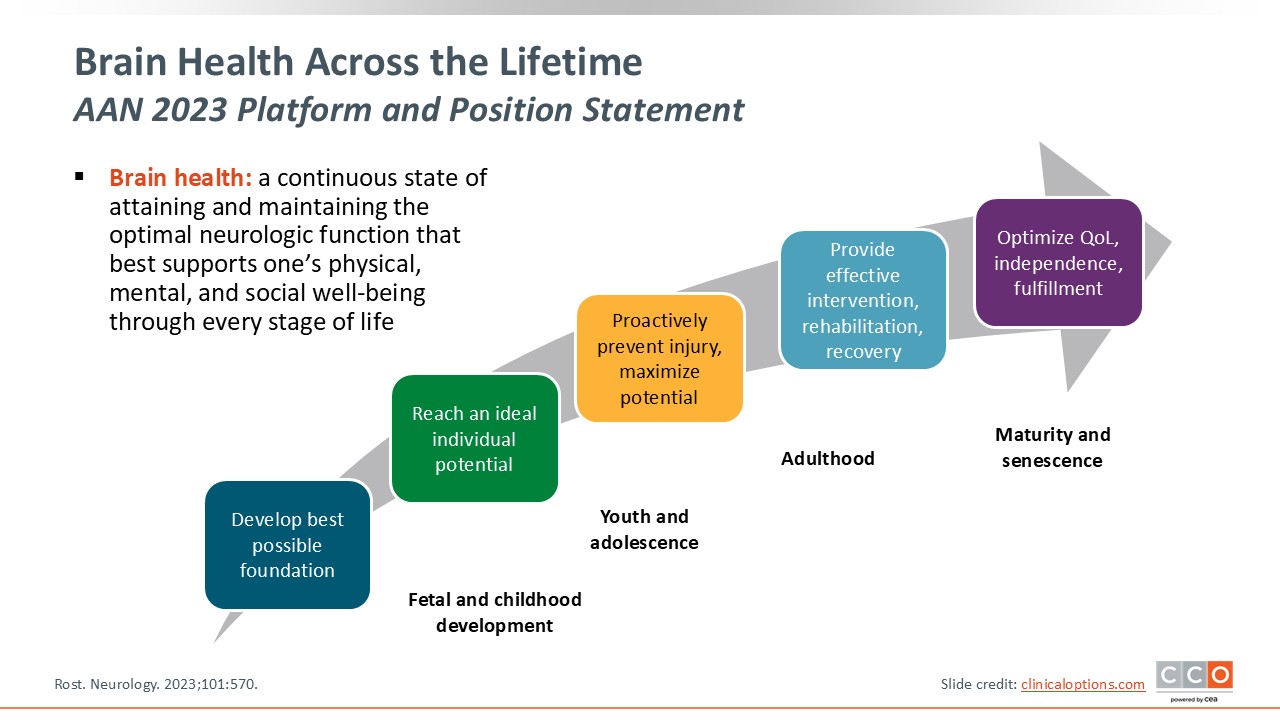
Brain Health Across the Lifetime
Alireza Atri, MD, PhD:
I am a cognitive neurologist, and like Dr Cohen, I am involved in patient care and mostly see early onset of AD and related disorders. I am also a clinical trialist and involved with the translation of recent advances into real-world practices. I endorse everything Dr Cohen said about the importance of the brain and its abilities.
In the field of dementia, we have recently made many strides forward with biomarkers and new classes of drugs. At the same time, we appreciate that by the time symptoms of dementia develop, the organ is already failing. Thus, we have great opportunities for prevention using everything in our arsenal, including brain health approaches and lifestyle changes.
Brain health approaches and lifestyle changes can not only add but potentially even synergize to help with care, treatment, and increased brain reserve. These are areas that I think all of us, as neurologists, are going to be involved in more and more. Whether it's the World Health Organization,1 the American Academy of Neurology (AAN),2 or others, the approach that will be emphasized in the coming decades is that of prevention and lifestyle changes.
The Current and Emerging Brain Health Crisis
Sharon Cohen, MD, FRCPC:
To build on Dr Atri’s point, we should not wait until the brain is already failing; we need to move earlier. With AD in particular, we are at a crisis point with a very serious disease that is increasing in prevalence such that almost 7 million Americans now have Alzheimer's and approximately 14 million will have it by 2060.3
It is unacceptable to have such an important part of oneself deteriorate due to AD. We fortunately know that the pathology of this progressive and ultimately fatal disease starts before any symptoms become apparent. This provides a tremendous window of opportunity for us to intervene. Accumulation of amyloid is the earliest brain change that we can detect; this occurs up to 20 years before symptoms emerge.4 We can improve outcomes by helping people act early, not simply waiting until they become symptomatic. However, another key imperative is not to ignore or minimize symptoms when they do occur; the earlier we can detect symptoms, the more we have to offer our patients.
Alireza Atri, MD, PhD:
That window of opportunity for intervention is crucial. We now have biomarkers that allow research into understanding what the drivers of AD are for any individual. Although we know that amyloid plaques and neurofibrillary tangles define the disease, we also appreciate that neuroinflammation, immune dysregulation, and vascular mechanisms accumulate and contribute to the pathology of AD. Other neurodegenerative proteinopathies are also often comorbid and further complicate the pathology in individual patients.5
In the context of resilience and vulnerabilities to biopsychosocial environmental characteristics, amyloid may be a more impactful driver of disease in some patients than in others. We have a foothold now with meaningful treatment options with our first-generation disease-modifying drugs, but we are likely to need additional combination approaches in the future to address the needs of all patients.
Current Clinical Trials in AD Prevention
Alireza Atri, MD, PhD:
The current approach of targeting amyloid plaques for treatment of AD has inspired a number of secondary prevention trials. Dr Cohen and I are involved with some of these, and our field is very much looking forward to the results.
First, the AHEAD 3-45 study is investigating the plaque-lowering monoclonal antibody lecanemab.6 This is a 2-arm trial in patients who are asymptomatic but have some level of amyloid plaques in the brain, divided into those with high or intermediate loads. Objectives are lowering of amyloid plaque and slowing or delaying progression to impairment.
Second, Trailblazer-Alz-3 is an ongoing secondary prevention study using donanemab, a different monoclonal antibody that works in a different part of the pathway (NCT05026866). It is also investigating the impact of treatment and amyloid plaque-lowering on the progression to symptoms, mild cognitive impairment, and dementia stages of AD.
Trials in dominantly inherited AD are being conducted by the Dominantly Inherited Alzheimer's Network Trial Unit (DIAN-TU) (NCT05552157). The Alzheimer’s Prevention Initiative (API) is also looking at different methods of plaque removal with potential to mitigate the progression of AD.7
Sharon Cohen, MD, FRCPC:
I am so excited about these secondary prevention trials. We know that primary prevention, largely lifestyle strategies, is also important. However, if we have interventions for individuals who already have amyloid accumulating in the brain but who are still cognitively well, we can potentially change their trajectory and keep them from developing dementia. That would be a huge win.
Phase III studies with donanemab8 and lecanemab9 in early symptomatic AD (mild cognitive impairment and mild dementia stages) have shown the ability to slow down the disease, to buy people more time, and to keep people at milder stages longer. In the lecanemab trial, the subgroup who were biologically earliest, with very low tau or low amyloid levels, tended to remain stable or even improve their cognition and function with lecanemab treatment.10 I believe we are on the cusp of really early intervention in AD. AHEAD will read out 3 years from now in 2028, which is just around the corner.
Alireza Atri, MD, PhD:
I am also very excited about the readouts of the secondary prevention trials. If they are successful, we will need to determine how best to communicate these benefits to people without symptoms but with elevated brain amyloid plaques, and to patients and families; and to set up the infrastructure for this type of care. In 3 years’ time there may well be other advances, such that these agents may be available as injections rather than needing to be infused.
Hopefully we will learn a bit more about monitoring for possible adverse events, such as amyloid-related imaging abnormalities (ARIA).11 These consist basically of leakiness and inflammation across blood vessels that can cause swelling or areas of microbleeding in the brain. Although ARIA is not symptomatic in most patients and can only be detected with imaging, it can become symptomatic and dangerous if not detected or managed promptly.
With an increasing number of patients potentially receiving these agents, translating treatment advances to real-world practice will require corresponding increases in proficiency, knowledge, cooperation, and system readiness. The currently available monoclonal antibodies provide valuable care for symptomatic patients with AD, but more work remains. Treatment of symptomatic AD is one arm, with the other arms being brain health and modifiable risk factors.
Sharon Cohen, MD, FRCPC:
I agree, I think that there will be a huge appetite for an intervention that can keep patients cognitively well, rather than waiting to treat cognitive impairment after it has begun. There is also space for ideas that have been adopted in some spheres but not implemented fully or consistently, such as including cognitive screening at every annual wellness exam. Having something tangible that allows us to intervene early will open a lot of opportunities for our patients.
AAN 2023 Platform and Position Statement
Alireza Atri, MD, PhD:
I think of this brain health imperative in the same way that I think of imperatives in cardiology. Preventive care has been really embraced and become an important part of cardiology practice, to the point that it ultimately has become part of primary care as well.
As neurologists, preventive care will also become a major part of our practice. Whether you are a cognitive or behavioral neurologist or a general neurologist, maintenance strategies for brain health are going to be very important for a vast majority of the conditions that we will face and need to address as the population is growing older.
In 2023, the AAN published a position statement on brain health as a key to neurologic health.2 This lays a foundation for collaboration between multiple disciplines across the lifespan, for the US and the rest of the world. Primary care HCPs are the quarterbacks in this plan, but neurology, cardiology, endocrinology, and even more specialties are included.
The statement elucidates goals of accelerating scientific discovery in brain health through cross-disciplinary collaborations, looking at optimization through integration of preventive practices, and enhancing public and patient engagement to advance public policy in this realm. It includes an outlined aspirational vision of brain health for 2050.
Sharon Cohen, MD, FRCPC:
I love the vision for 2050 from the AAN. By that time, they envision having a very robust body of research-derived knowledge and scientific breakthroughs, leading to a thriving preventative neurology field spanning multiple disciplines. That is a very positive outlook for the future. We want to practice with evidence-based guidelines to aid us in brain health. We want brain health visits to be the standard of care at wellness visits across the lifespan, not just when people reach an age where cognitive impairment becomes more likely.
Education on brain health is going to be important; many stakeholders will need to be engaged and involved in a National Brain Health Plan with the goal of establishing a guide to scientific research, care, and public engagement priorities. This is extremely aspirational, but if we all take part in chipping away at the end goal, we can make it a reality. The brain is such an amazing organ, and we can easily take it for granted until it stops working.
It might be helpful to compare that future vision with the current standard of care for people presenting with cognitive concerns. Unlike primary care HCPs who follow patients over long periods of time, neurologists may see a patient just a few times for a very specific reason, such as migraines or numb hands due to carpal tunnel syndrome. How do you insert a conversation about brain health into these visits?
You can embark on a discussion by directly asking, “How is your memory? How is your brain health?” You can also keep literature and posters in the waiting room for patients to take away or look at while they are in the clinic. There are many ways to educate our clientele even without direct discussions about brain health.
Alireza Atri, MD, PhD:
We should also consider how to set the stage, as the AAN has, that brain health is an important part of a holistic approach to the neurology patient in the same way that primary care considers the annual wellness visit. If a patient who comes to the neurology clinic with a neurologic issue, maybe regular neurologic wellness visits should be scheduled throughout the lifespan for continued monitoring of brain health, even if not as often as every year.
One problem is that neurologic preventive care has been given the short shrift. We need to have these discussions across the lifespan, particularly in midlife. A body of data shows that patients with AD have, on average, a milder course of disease later in life if their blood pressure and diabetes have been well controlled.12,13
Multidisciplinary Support for Dementia Specialists
Sharon Cohen, MD, FRCPC:
It is challenging because the nature of neurologic practice does not lend itself to opportunities for preventative discussions. Certainly, in Canada, it is not happening regularly, even in primary care settings. Family physicians are already stretched too thin and adding brain health discussions and cognitive testing to their existing workload would be asking a lot. However, HCPs don't want to miss a treatment opportunity. If there are effective preventive strategies for a very serious disease, HCPs will reorganize their priorities to accommodate them. This will also bolster the opportunity to talk about lifestyle strategies throughout the lifespan and even in the face of already present disease. For example, being able to sleep better and exercise will improve a person’s quality of life even if they have moderate dementia.
We need to advocate aggressively to make the case that lifestyle strategies matter and that the population is going to be healthier because of them. We can draw on examples from cancer medicine where specific lifestyle strategies are viewed as worthwhile. Regarding brain health, patients and family members are often eager to explore lifestyle factors and have many questions for us. There may be lengthy conversations with individuals who want to know about different types of diets, the value of quality sleep, or what kind of exercise is the right exercise to help the brain. Tailoring a conversation to an individual and their interests is required; it is not as simple as handing out a list of 10 things everyone should do.
This can be time-consuming within a clinical visit. However, there may be an opportunity for allied HCPs, including physician associates and nurse practitioners, to take on patient education. We might also consider offering workshops that patients can attend. Advocacy organizations are providing some of these opportunities.
Financial Barriers for Testing and Treatment
Alireza Atri, MD, PhD:
Ultimately, we know that conversations about brain health can be impactful. There are 5% or 10% of patients who listen and adopt immediately, but the vast majority of people need to hear things more than once and need help to find ways of fitting these changes into their lives. You have to pick your battles, come up with plans, problem solve with them, and encourage them. It is an ongoing conversation. Hopefully, they will hear similar messages from their cardiologists and primary care HCPs as well, so the totality of that messaging is more impactful.
As far as reimbursement, I integrate brain health approaches and lifestyle as an absolute pillar into all my clinical visits. I explain in multiple ways that brain health affects a patient’s biology, mental health, and sleep, as well as linking back to what it potentially means in terms of the future course of their AD. For example, on the topic of sleep, I mention that the brain removes amyloid during certain phases of sleep.14 As we get into the habit of weaving mentions of brain health into our visits, we aspire that payers will ultimately cover these discussions on their own merits. As Dr Cohen mentioned, group sessions or team care may also help play a role in education.
Implementation of Brain Health Discussions in Practice
Sharon Cohen, MD, FRCPC:
I see many family members who accompany their loved ones to clinical visits who are interested in their own brain health. Sometimes, the family member is quite burdened by providing care and they need help to relieve stress and make time for their own brain health. The adult children and even grandchildren of my older patients are often very interested in what actions they can take for themselves to avoid the disease they are seeing in their loved one. Again, it can be a challenge to give them the time they deserve to discuss a complicated topic and not just pay lip service to it. I often address their questions briefly and then say, “If you would like to go into this in more depth, why don't we make a separate appointment just to discuss these issues?” From a billing perspective, I can bill that next visit as a counseling session, which allows me to devote the appropriate time.
Facilitating local connections can also be helpful. Specialized services such as lifestyle coaches, personal trainers, smoking cessation programs, or alcohol addiction services can be useful for some patients, particularly if you have referral information to provide. Again, these are not one-size-fits-all solutions.
Alireza Atri, MD, PhD:
I also take the opportunity whenever I can to talk with care partners about brain health strategies. Family members of people with dementia often carry a fair degree of burden and stress, which compromises their own health. I always explain that the patient and care partner function as a unit, and that caring for the care partner is imperative as it impacts the well-being of the primary patient.
I try to collaboratively brainstorm ways that the care partner can get their own respite, perhaps in some activity that can benefit them both, such as going to the mall to walk together. Then, on the next visit, I inquire how well these ideas have worked. The goal is that they won’t perceive a huge mountain they have to climb, but rather small things that they can easily start and take on one at a time. What can be manageable as the next bite-sized step for them?
Sharon Cohen, MD, FRCPC:
I like to get to know my patients. What are you interested in? What hobbies do you have, or would you like to get back to? What resources can we rely on? The Alzheimer Society and its chapters have many social programs, such as trips to the museum or discussion groups. These are opportunities for care partners to get out, socialize, and engage in something mentally stimulating. This doesn’t cover all 14 Lancet Commission brain health strategies, but it does include several, which is a good start. It is important to remember to “do what's doable” if it will benefit the patient in front of you.
Risk Factors for Dementia
Alireza Atri, MD, PhD:
Dr Cohen mentioned the natural progression of AD. In some sense, any type of brain injury—whether vascular, traumatic, ischemic, or another mechanism—potentially decreases reserve and may synergize with neurodegenerative pathways related to dementia.15 While we don't have definitive proof, neuropathology studies of individuals with multiple types of brain injuries suggest these damages may have additive or even multiplicative effects on the rate and severity of cognitive decline.
Our predictive population models are not great at indicating risk for the individual patient in hard numbers over the next 3, 5, or 10 years. However, they are quite clear on positively vs negatively impactful factors. Modification of cerebrovascular risk factors and mitigating other risk factors such as diabetes, smoking, blood pressure, and cholesterol are plainly beneficial. Again, getting to know the individual patient and finding out their values helps substantially in finding approaches, strategies, and interventions that are consistent with their personal goals.
Predictors of Brain Health
Alireza Atri, MD, PhD:
Throughout a lifetime, a number of biologic, environmental, and other factors allow people to process information more efficiently and potentially become more resistant and better able to repair and overcome neuropathologic damage. This reserve allows a certain level of cognition to be maintained in the face of some level of injury to the brain.
Sharon Cohen, MD, FRCPC:
I tell my patients that more brain cells and more connections between brain cells are part of a bigger, healthier brain. Cognitive engagement, physical exercise, and other lifestyle modifications help brain cells work optimally. When I went to medical school, I learned that you are born with a certain number of brain cells, and it's all downhill after that. We now know that’s not true and that we can grow new brain cells, given the right environment and the right stimulation, particularly in the hippocampus.16 Furthermore, the entire brain has potential to sprout new connections, which enlarge brain cell networks.17 In the case of an injury or neurologic disease that damages brain cells, starting with a bigger, healthier organ allows more resilience and the ability to mitigate damage and preserve function. I’ve found that this type of explanation resonates with my patients and provides them with a rationale for embracing brain-healthy lifestyle strategies.
Staging the Cognitive Continuum
Sharon Cohen, MD, FRCPC:
AD is a complex disease with a long clinical continuum and an even longer biologic continuum. The earliest stages of AD are clinically silent, with either no cognitive impairment or some subtle complaints that don’t rise to the level of abnormality on formal assessment. This doesn’t mean that no impairment is present, it just means that our clinical tools are not sensitive enough to detect it.
From this so-called cognitively unimpaired stage, patients with underlying AD brain changes will progress to a stage of mild cognitive impairment. Here, the individual has a complaint about cognition, often memory but sometimes language or another domain, and objective evidence of impairment on cognitive testing. This impairment is not of a magnitude that significantly impacts an individual's ability to function, that is, they are still independent in banking, shopping, driving, cooking, traveling, and whatever it is that constitutes their usual daily activities. They may, however, experience frustration, and feel they are slower or need to rely more on notes or other compensatory strategies, but they are still independent.
After an average of 5 years of mild cognitive impairment due to AD, patients seamlessly progress to the dementia stage, which is often broken down into mild, moderate, and severe dementia. This stage includes increasing loss of functional independence, increasing decline in cognition across multiple domains, and more complex and challenging neuropsychiatric symptoms.
How Is AD Currently Defined?
Alireza Atri, MD, PhD:
The field has evolved in what we commonly include within the definition of AD. Ten to 15 years ago, the term “Alzheimer's disease” almost always referred to the clinical syndrome of dementia with the Alzheimer's type, as we had no biomarkers at the time. Now, there has been a movement to consider biologic AD as including detectable biomarkers even at stages where individuals may not have clinical symptoms. We have 2 schools of thought, with more in common than not.
In 2024 the Alzheimer's Association and the International Working Group each released revised criteria for AD.18,19 The Alzheimer's Association made the change of defining AD entirely by biomarkers without requiring demonstration of clinical symptoms. This definition had previously been used for research purposes, but they now considered it applicable to clinical practice as well. The presence of either amyloid β proteinopathy or phosphorylated and secreted tau was sufficient as a CORE 1 biomarker to diagnose AD, even in patients with no symptoms. That caused a little bit of controversy in our field, as the International Working Group responded by publishing criteria that are a little less far-reaching. These considered the definition of AD to remain a clinical–biologic construct, including cognitive deficit as well as biomarkers to be present for a clinical diagnosis.
Despite the difference in diagnostic criteria for AD itself, both groups agree that the use of biomarkers for detection of patients who are in the biologic stages of the pathway but have not yet developed a clinical presentation is key to prevention, regardless of whether one considers these patients to have AD as such.
Available AD Biomarkers
Alireza Atri, MD, PhD:
There is recognition that the presence of amyloid plaques is a risk state for progression to cognitive impairment over years or potentially a decade, compared with those without plaques.20 The data have suggested that once tangles appear in addition to plaques, it is almost like introducing fire to an accelerant, which is the amyloid. That's a very high-risk state. As tangles continue to develop with higher staging, increased density, and severity of topographic spread, those individuals have a very high risk of progressing to impairment or dementia over the next 3 to 5 years.
This is a really exciting new era in which we can now actually measure some of these biomarkers in multiple ways, meaning that we can think about the biology and syndromes on different spectra.21 The multiple PET, spinal fluid, and blood biomarkers have different temporal courses and sensitivities, reflecting subtleties of disease progression that were not visible to us previously.
Alzheimer's Association DETeCD-ADRD Clinical Practice Guideline 2024
Alireza Atri, MD, PhD:
Another exciting development within the last year is that the Alzheimer's Association, through an Institute of Medicine and modified-Delphi guided process, completed the 7-year process of creating clinical practice guidelines. This was done through the review of over 7000 papers, rigorous evidence grading and assessment, and recommendation development. Professor Brad Dickerson and I were co-chairs of this multidisciplinary work group, which did not only include cognitive neurologists but comprised representation from primary care, geriatrics, nurse practitioners, neuropsychology, geriatric psychiatry, and other specialties.
The work group established 19 recommendations for the evaluation of patients with suspected AD and related dementias in a process flow that was formalized for primary care, secondary specialty care, and subspecialty care.22 The recommendations are centered around discussing establishing goals and defining investigations with the patient and care partner in a personalized and formalized process. What are the elements of history? What are the structured domains and systems reviews? What are the risk factors? What are the components of an exam? What are the instruments?
Integrated into the context of all the historical information, the initial workup should also involve at least 1 standard validated cognitive exam to establish, with a high level of confidence, that this person is either cognitively unimpaired or that there is a potential and concerning change or impairment warranting further investigation. The next step should be characterize their cognitive syndrome, such as whether it involves memory, language, both, or other domains, and their level of functional dependence. And next, to consider diseases and conditions that may be causing or contributing to the cognitive syndrome. Tiers of testing are delineated. When do you consider them? When do you order labs and imaging? What tests and what modality? What about spinal fluid? Genetic testing? When should you refer for neuropsychological evaluation?
These recommendations are not criteria in the pure sense; they refer to different criteria from different groups for etiologies beyond AD, such as Lewy body or vascular dementia. Resources are provided, including scripts for discussing and disclosing a diagnosis with patients and families, descriptions of instruments with links for use, tips on daily activity and living behavior, and much more. The recommendations are a valuable resource that should be practical to use and are available now in an open-access special edition of the Journal of Alzheimer's and Dementia.
Sharon Cohen, MD, FRCPC:
I think these recommendations are excellent, and I must say that the part that I like best is that CORE 1 and CORE 7, the first and last recommendations, are very patient-centered. Speak to your patient. Why are we doing this investigation? Do we agree that this is worth pursuing? Finally, what have we learned? Here is my understanding of your diagnosis and my recommendations. What next steps shall we take together?
The importance of patient communication seems so obvious, but as HCPs we are sometimes so busy checking off lab requisitions and ordering tests and scans that we neglect the person in front of us. We are taking them on a journey, and we should ask ourselves whether we have explained to them why we are doing certain tests and asking certain questions. Similarly, we should ensure we spend adequate time explaining what we’ve found and what their next steps might be. I am always dismayed when I find a patient who has not even been told their diagnosis although it is written in their physician's chart.
Alireza Atri, MD, PhD:
We did not aim to create more clinical work, but to empower patients, families, and clinicians to ask for the necessary resources to implement these guidelines within the US healthcare system. With improved knowledge, tools, and resources, HCPs will hopefully be able to more effectively and efficiently go through the processes described to empower patients and families with the autonomy to make their choices heard.