
CE / CME
Nurse Practitioners/Nurses: 1.00 Nursing contact hour
Pharmacists: 1.00 contact hour (0.1 CEUs)
Physicians: maximum of 1.00 AMA PRA Category 1 Credit™
Released: August 21, 2024
Expiration: August 20, 2027
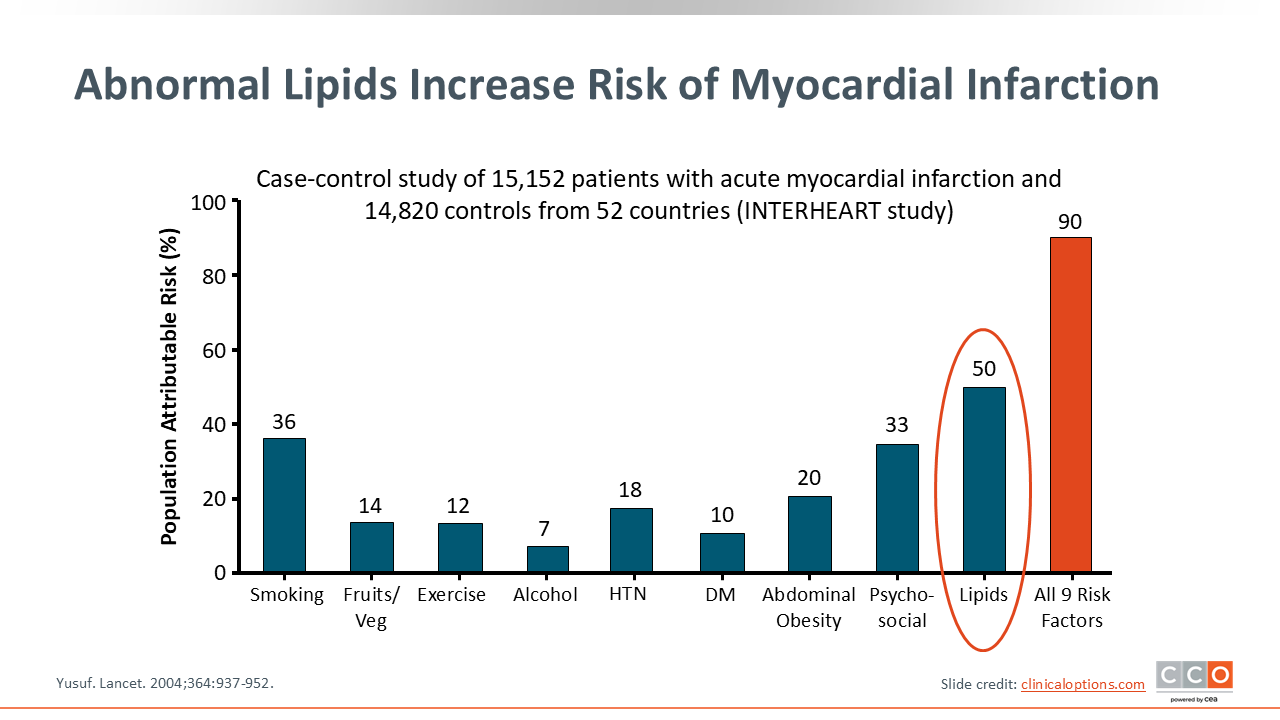
Abnormal Lipids Increase Risk of Myocardial Infarction
Let’s begin by reviewing the current approach to managing hyperlipidemia. Cardiovascular disease (CVD) is the leading cause of death in the United States for both men and women.1 Despite significant investment in cardiovascular health, the rates of CVD continue to rise.2 Hyperlipidemia remains a prominent traditional risk factor, often ranking higher than hypertension, diabetes, and psychosocial stressors, which are also closely linked to cardiovascular risk.3 This program will focus on effectively diagnosing elevated cholesterol levels and, more importantly, how to manage them aggressively. As we proceed, we will gain a clearer understanding of these strategies.
Why LDL Lowering Is Important: Cumulative LDL-C Yr vs Age
Lowering LDL-C is crucial because LDL is the most atherogenic type of cholesterol. Strong evidence supports that LDL and other apolipoprotein B (apoB)-containing lipoproteins are directly responsible for the atherogenesis.4
Cumulative cholesterol exposure at various ages is also significant. In younger individuals, the focus is often on hereditary components, such as familial hypercholesterolemia (FH). FH is a genetic condition that can manifest as either homozygous or heterozygous forms, leading to elevated cholesterol levels from birth and significantly increasing the risk of CVD early or later in life.4
As we age, moderate hypercholesterolemia can develop due to genetic factors or lifestyle choices. Traditional risk factors like obesity, which is increasingly prevalent among teenagers, also contribute to elevated cholesterol levels. This trend continues into adulthood, where cholesterol issues persist and can even appear in people following good lifestyles or with lower LDL levels, potentially due to favorable genetics.5
Cholesterol impacts us at every life stage, even in utero.6,7 Understanding and managing LDL levels across these stages is essential for reducing cardiovascular risk throughout life.

Statins Remain Mainstay Therapy for Key Risk Groups
When considering treatment options for lowering cholesterol, statins are recognized as the mainstay of pharmacotherapy.8 However, the foundation of managing hyperlipidemia begins with lifestyle modifications. Therefore, our initial focus will be on these lifestyle interventions.
According to the American Heart Association (AHA), engaging in at least 150 minutes of moderate cardio exercise per week is recommended. In addition, we will emphasize the importance of a heart-healthy diet.9 Once it is determined that a patient requires pharmacotherapy, statins often become the cornerstone of treatment.
Visual data clearly demonstrate that lowering LDL-C is beneficial for both primary prevention (patients without evidence of atherosclerotic cardiovascular disease [ASCVD]) and secondary prevention (patients with existing ASCVD). As LDL levels decrease, the risk of major adverse cardiovascular events (MACE), such as myocardial infarction or cardiovascular death, also declines.10 Therefore, our objective is to reduce LDL levels as much as possible, tailored to the individual's risk profile.

Statin Intensity and LDL-C Reduction
Intensity of statin therapy is an important concept to review. High-intensity statins are often utilized in secondary prevention. These are typically prescribed to patients who have recently experienced a myocardial infarction, stroke, or symptomatic peripheral arterial disease. Examples include atorvastatin at doses of 40 to 80 mg and rosuvastatin at doses of 20 to 40 mg.8
There is also a broader category of moderate-intensity statins with many dose-specific options available. We will delve into the guidelines to determine when to initiate moderate- vs high-intensity statin therapy.
It is also important to recognize that not all statins are created equal. Statins may possess lipophilic or hydrophilic attractions, which further determine metabolism and tissue-selectivity characteristics.11 Understanding these differences can be beneficial, especially for patients who may experience side effects from statins.

Despite Statin Therapy, Residual Risk Remains
It is important to understand that despite statin therapy, that there could still be a residual risk that remains. The trials shown in this slide depict the CVD risk-reduction by statin treatment compared to placebo for key secondary and primary prevention lipid trials. Across all the studies shown, events are reduced but not completely eliminated and we call this residual risk. The residual risk can vary widely, ranging from 0.8% to as high as 19.4%, depending on the specific study.12-18
This residual risk isn't solely due to lipid-related factors. Emerging evidence suggests that elevated levels of lipoprotein(a) [Lp(a)] could also play a significant role. In addition, the suboptimal control of other risk factors, such as hypertension, diabetes, or smoking, can contribute to this remaining risk.19 Recognizing and addressing these factors is crucial for comprehensive cardiovascular risk management.

2018 Blood Cholesterol Guideline Recommendations
In 2018, the American College of Cardiology (ACC) and AHA Task Force on Clinical Practice Guidelines provided recommendations for the management of blood cholesterol within key patient groups. Clinical ASCVD encompasses patients with a known history of disease. Patients with severe hypercholesterolemia have LDL-C levels ≥190 mg/dL. Adults with diabetes must take into consideration age and time with the disease. The focus of this education will be on primary prevention, which explores prevention based on an assessment of risk factors.20

What’s New From the 2022 ACC ECDP on the Role of Nonstatin Therapies to Reduce ASCVD Risk?
Since then, the ACC has released an Experts’ Consensus Decision Pathway to help appropriately utilize nonstatin therapies, including guidance on when to add bempedoic acid, evolocumab, or inclisiran.21 Each contributes a notable impact in reducing cardiovascular outcomes given current data.

Many LDL-C–Lowering Tools at Your Disposal
There are many new LDL-C–lowering medications now available. Recent evidence not only shows their efficacy in managing hypercholesterolemia, but they appear to offer promising ASCVD benefits.22

Intestinal Cholesterol Absorption Inhibitor: Ezetimibe
Ezetimibe works by decreasing the intestinal absorption of cholesterol. It is FDA-approved as monotherapy, administered orally once daily, and has been shown to reduce LDL-C by as much as 18%.22 The IMPROVE-IT trial added ezetimibe to simvastatin treatment, resulting in an additional reduction in LDL-C by 24%.23 It is not for use in patients with moderate or severe hepatic impairment.24

IMPROVE-IT: Ezetimibe Efficacy
Ezetimibe opened our eyes to the possibilities offered by nonstatin therapies in terms of cardiovascular outcomes. With the IMPROVE-IT, adding ezetimibe to simvastatin therapy reduced the absolute risk of composite of cardiovascular death, nonfatal myocardial infarction, unstable angina requiring rehospitalization, coronary revascularization, or nonfatal stroke by 2 percentage points compared to simvastatin alone.23 This allowed us to rethink the potential for nonstatins to not just reduce cholesterol, but also have overall positive ASCVD effects.

PCSK9 Inhibitor mAbs: Alirocumab and Evolocumab
Soon after, interest developed in proprotein convertase subtilisin/kexin type 9 (PCSK9) as a mediator of LDL-C regulation. PCSK9 inhibitors were initially approved by the FDA for use with a statin to manage hypercholesterolemia, though studies eventually proved their effectiveness in reducing the incidence of MACE.22 As add-on therapy with statins, alirocumab reduced the baseline LDL-C by 48% at 12 weeks, while evolocumab achieved 63% to 71% reductions. Each is now approved as monotherapy in adults, and we will discuss studies that allowed their labeling to include indications for the secondary prevention of MACE.25,26 Both are injected subcutaneously every 2 to 4 weeks, and injections site reactions are the most common adverse event. Despite concerns about an increased risk of developing new-onset diabetes, no clinical trial data currently supports this.22 However, we should always be mindful of hemoglobin A1C when starting patients on any lipid-lowering therapy.

PCSK9 Inhibitor Monoclonal Antibodies: Impact on MACE
Two pivotal studies for the PCSK9-inhibitors gave us evidence of their ability to reduce MACE: the FOURIER trial and the ODYSSEY trial.22 FOURIER showed that evolocumab in patients with ASCVD reduced the risk of MACE to 12.6%, as compared to 14.6% for the placebo arm (95% CI: 11.7-13.5; P = .0001).27 Results were similar in the ODYSSEY study with alirocumab. When utilized with the highest intensity statin, MACE risk was reduced compared to placebo (12.0% vs 14.2% [95% CI: 0.74-0.94; P = .003]).28

FOURIER-OLE: Lower for Longer Is Better!
When the FOURIER study ended, patients were allowed to continue in open-label extension trials (FOURIER-OLE) such that all participants could now receive evolocumab. Of interest, results showed that, for those who had received evolocumab from the beginning, the overall risk reduction was greater than that seen with patients transitioning from placebo to active drug despite similar LDL-C levels at Week 12. The primary outcome of MACE differed significantly for those originally randomized to evolocumab than placebo (HR: 0.85; 95% CI: 0.75-0.96; P = .008). So the question of early initiation, for example, immediately upon the occurrence of an acute myocardial infarction now appears to be yes, but there are always some challenges when it comes to insurance coverage.29 But it is very positive to demonstrate that the earlier we lower that LDL-C, the better the outcomes would be.

ATP-Citrate Lyase Inhibitor: Bempedoic Acid
Now we're going to change gears a little bit to talk about bempedoic acid and how it compares to statins. While PCSK9 inhibitors are blocking LDL receptors on liver cells, bempedoic acid and statins work to reduce production of cholesterol altogether. Bempedoic acid blocks a key enzyme upstream to HMG-CoA reductase.22 Phase III studies showed that bempedoic acid added to statin therapy significantly reduced LDL-C levels at Week 12 by an additional 16.5% and 15.1% respectively, compared to placebo.22,30 It is important to note that bempedoic acid is a prodrug and the enzyme responsible for its conversion to an active metabolite is expressed in liver cells but not muscle cells.30 As a result of that, it would be very uncommon to have any muscular side effects. It is a daily oral agent that was initially FDA-approved for LDL-C lowering but a recent label change contains an indication for the reduction of ASCVD risk in adults who cannot tolerates statins in the presence of CVD or at high risk for a CVD event.22,31 Bempedoic acid can increase serum uric acid levels, so it should be used with caution in patients that have a history of gout. There is some risk of tendon rupture as well.31 These are things to be mindful of when thinking about which patients would benefit.

CLEAR Outcomes: Bempedoic Acid CVOT
The CLEAR Outcomes trial explored potential cardiovascular benefits with bempedoic acid in statin-intolerant patients with ASCVD or who were at risk of a CVD event. For the total population, the risk of MACE was significantly lower with bempedoic acid than with placebo (11.7% vs 13.3% [HR: 0.87; 95% CI: 0.79-0.96; P = .004).32,33

PCSK9 mRNA Synthesis Inhibitor: Inclisiran
The PCSK9 inhibitors presented thus far inhibit PCSK9 from binding to the LDL receptors through monoclonal antibody binding to PCSK9. An additional mechanism to block the PCSK9 pathway involves using a small interfering RNA to interfere with its production. This is administered as a subcutaneous injection which, after the first 2 doses, can be given every 6 months. This may be most useful for patients who may possibly have concerns about compliance. For example, they travel a lot and it's hard for them to remember to take something refrigerated with them. I will say that to date it has demonstrated a lot of great success. So we're seeing that we were able to achieve a 49% to 56% reduction in LDL-C lowering, which has been extremely impactful, though we don't have our cardiovascular outcomes data yet.22 Inclisiran was approved by the FDA as an adjunct to diet and statin therapy for the treatment of adults with primary hyperlipidemia, including heterozygous FH, in 2023.34

ORION-10: Clinical Efficacy of Inclisiran in Patients With ASCVD on Maximally Tolerated Statin Therapy
Here are some of the data that we’ve seen so far on inclisiran with the ORION-10 trial. We can see that there is notable lowering and percent change in LDL in those who are either on placebo vs inclisiran.35


