
CE / CME
Nurse Practitioners/Nurses: 1.00 Nursing contact hour
Pharmacists: 1.00 contact hour (0.1 CEUs)
Physicians: maximum of 1.00 AMA PRA Category 1 Credit™
Released: August 21, 2024
Expiration: August 20, 2027
ASCVD Prevention Risk Groups
We will now shift focus to individualizing and implementing therapy to achieve LDL-C goals in 4 key patient groups: those with clinical ASCVD, those with diabetes, those with primary severe hypercholesterolemia, and those with none of these conditions.20

Criteria for Defining “Very High–Risk” ASCVD
For patients with known ASCVD, there are new criteria that help us define patients at very high risk vs high risk in determining the role of nonstatin therapies. To be considered very high risk, a patient would have had 2 major ASCVD events, or 1 in combination with 2 or more high-risk conditions. An ASCVD event needs to have occurred within the past 12 months, or there should be a history of myocardial infarction, history of ischemic stroke, or symptomatic peripheral artery disease. High-risk conditions that contribute to the overall “high-risk” assessment include older age, chronic kidney disease, a history of bypass surgery or percutaneous intervention, smoking, diabetes status, a history of heart failure, hypertension, or LDL-C ≥100 mg/dL.21

Thresholds for Initiation of Nonstatin Therapy in ASCVD
A new ACC Expert Consensus Decision Pathway from 2022 indicates a much lower LDL-C cholesterol threshold for adults with ASCVD. Rather than ≤70 mg/dL, the recommendation is now ≤55mg/dL. This is echoed in the European Society of Cardiology recommendations as well. Without the presence of ASCVD, the LDL-C target remains ≤70 mg/dL. For adults with ASCVD plus a baseline LDL-C >190 mg/dL and no FH, the goal also is ≤70 mg/dL. Since FH leads to a robust increase in an individual’s risk of atherosclerosis as a genetic condition, the target is more aggressive at ≤55 mg/dL.21

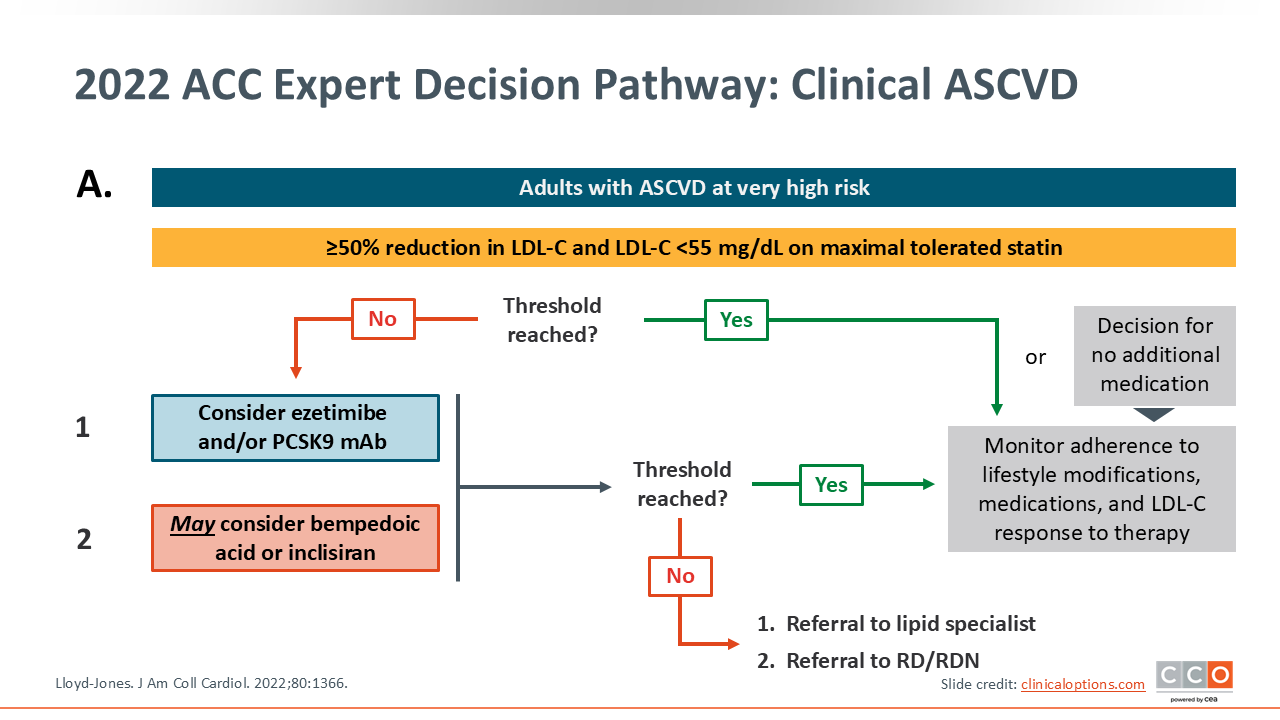
2022 ACC Expert Decision Pathway: Clinical ASCVD
When we cannot reach these goals, other agents can be considered, including ezetimibe or PCSK9 inhibitors as the preferred therapies, and bempedoic acid or inclisiran as alternatives. Shared decision-making and the consideration of outside factors, such as insurance coverage, are important conversations.21
2022 ACC Expert Decision Pathway: Clinical ASCVD
There are minor modifications in recommendations for patients who are not considered very high risk, including a preference for ezetimibe over other treatments.21

ACC ECDP: Thresholds for Initiation of Nonstatin Therapy
For patients without ASCVD whose baseline LDL-C is ≥190 mg/dL, the recommended goal is a reduction in LDL-C to ≤100 mg/dL.21 If this cannot be achieved with a statin, nonstatin therapies can be considered.

2022 ACC Expert Decision Pathway: Primary Severe Hypercholesterolemia
The initial goal in all scenarios is to use a maximally tolerated statin. As noted, if LDL-C goals cannot be reached with high-intensity statin, other options may be considered. The first-choice line of therapy is ezetimibe, followed by PCSK9 inhibitors, then bempedoic acid. In the setting of homozygous FH, there are other agents to be considered that may be best addressed through a visit to a lipid specialist.21

Estimating Cardiovascular Risk in Diabetes to Determine Statin Intensity
For patients that do not have ASCVD, there is value in calculating the atherosclerotic cardiovascular risk equation, particularly if they have evidence of diabetes. Based on older guidelines, everyone should be initiated on moderate intensity statins if they are between the ages of 40 and 75 with diabetes.47 We know that some patients with diabetes may be at a higher risk and a higher intensity statin could be initiated early in therapy. Risk calculators, as shown here, help guide decisions about starting therapy.48

Additional Risk Factors That Inform Diabetes Risk
Specific risk enhancers need to be factored in for patients with diabetes because we know that longer exposure to diabetes increases cardiovascular risk. These include a long duration of diabetes as well as evidence of organ involvement, as demonstrated by albumin in the urine, declining estimated glomerular filtration rate, retinopathy, neuropathy, or signs of peripheral arterial disease.20

Patients With Diabetes, but no ASCVD and an LDL-C <190 mg/dL
Based on current guidance, if the calculated 10-year ASCVD risk is 7.5% to 19.9% and a moderate intensity statin did not decrease LDL-C by 30% to 49% to ≤100 mg/dL, then a high-intensity statin should be instituted. If the 10-year ASCVD risk is calculated to ≥20%, high-intensity statin therapy would be recommended to target a goal LDL-C of <70 mg/dL.21

Estimating Cardiovascular Risk for Those Without DM
Upon revisiting the risk calculation, note that it is important for those that do not have diabetes as well. Calculating the ASCVD risk allows us to determine whether to initiate pharmacotherapy in a setting of borderline or intermediate risk.48

Using Coronary Calcium to Refine CV Risk Assessment
There is a lot of value in imaging as well. Luckily, we have that through the coronary artery calcium (CAC) score, which is a noncontrast CAT scan that is a marker of subclinical atherosclerosis. This is a screening test that should not be used for people with symptoms; for symptomatic patients we would use a different imaging modality. But as a screening test, the CAC score tells us an individual’s total plaque burden and ASCVD risk.20
Obtaining a CAC score is not invasive, often of low cost, and can help to identify patients at very high risk at the earliest points in their disease. The goal is for patients not to have any evidence of coronary atherosclerosis from calcified plaque, but for screening purposes, a calcium score is a good first step to better determine where are. More important, it is a good marker that can equate to those that are at lower risk vs higher risk and help to guide pharmacotherapy.

Primary Prevention Patients Who May Benefit From CAC
There are several groups of patients who benefit from learning that they have a CAC score of zero. First are patients reluctant to initiate statin therapy who wish to understand their risk and potential for benefit more precisely. Next are patients concerned about the need to reinstitute statin therapy after discontinuation. In addition, older patients with low burden of risk factors and middle-aged patients with a calculated ASCVD risk in the borderline group of 5% to 7.5% can benefit as well.20

2022 ACC Expert Decision Pathway: Primary Prevention
In the 2022 expert decision pathway for primary prevention, the goal for patients who have a 10-year ASCVD risk of 5% to 19.9% is a reduction in LDL-C by 30% to 49%, for an LDL-C <100 mg/dL. These patients should initiate a moderate-intensity statin and then increase to a high-intensity statin if needed to achieve their goal. Similar to patients with diabetes, if the risk is high, meaning that 10-year ASVD risk is >20%, patients should initiate treatment with a high-intensity statin with nonstatin therapy added if needed to achieve their goal levels.21


