CME
Physicians: Maximum of 1.50 AMA PRA Category 1 Credits™
Released: March 04, 2025
Expiration: September 03, 2025
Phase IV PADMA: ET Plus Palbociclib vs Standard Chemotherapy in High-risk, HR-Positive/HER2-Negative mBC
Heather McArthur, MD, MPH:
Moving on to data presented for patients with HR-positive/HER2-negative ABC.
At SABCS 2024, we saw the results from the prospective, multicenter, randomized phase IV PADMA study evaluating the combination of ET plus palbociclib vs physician’s choice of chemotherapy with or without ET maintenance therapy, in men and women with HR-positive/HER2-negative mBC and an indication for single-agent chemotherapy (N = 150).11
International guidelines have recommended ET with a CDK4/6 inhibitor as a standard first-line approach in this population. But because of the lack of prospective data comparing ET with SoC chemotherapy, many patients continue to receive chemotherapy as their first-line therapy. The primary endpoint of the PADMA trial was time to treatment failure (TTF, defined as time to discontinuation caused by disease progression, treatment toxicity, patient preference, or death).
PADMA: Baseline Characteristics
Heather McArthur, MD, MPH:
Baseline characteristics were balanced between the arms. The median age in the patient population was approximately 62 years. Most patients (~90%) were postmenopausal, approximately 42% had liver metastases, and approximately one third had ET-resistant disease (~32%).
Pathogenic variants included PIK3CA mutations (22.5%) and BRCA1/2-associated breast cancer (5.8%), with relatively low rates of ESR1 mutations—presumably because these patients had not yet received AI therapy.
PADMA: Treatment Exposure (as Treated)
Heather McArthur, MD, MPH:
Regarding treatments of physician’s choice, most physicians selected capecitabine chemotherapy (69%) and 22% received ET maintenance after chemotherapy. Other chemotherapy options were paclitaxel (29.3%) or vinorelbine (1.7%). Most patients received an AI (15.5%) as their ET, which is in alignment with the current SoC. Other ETs considered were tamoxifen (5.2%) and fulvestrant (1.7%).
PADMA: TTF (Primary Endpoint)
Heather McArthur, MD, MPH:
The PADMA study met its primary endpoint of improving TTF, with a median TTF of 17.2 months vs 6.1 months (hazard ratio: 0.46; P <.001) in favor of palbociclib with ET vs physician’s choice of chemotherapy followed by ET maintenance.
TTFs in subgroups were consistently in favor of palbociclib plus ET vs physician’s choice of chemotherapy regardless of the subgroup interrogated.
PADMA: PFS and OS (Secondary Endpoints)
Heather McArthur, MD, MPH:
We also saw improvement for the secondary endpoints of progression-free survival (PFS) and OS.
The mPFS was 18.7 months in the palbociclib plus ET group and 7.8 months in the chemotherapy group (hazard ratio: 0.45; P <.001). Median OS was 46.1 months with palbociclib plus ET and 36.8 months with chemotherapy.
PADMA: Safety Summary
Heather McArthur, MD, MPH:
No new safety signals were identified and the toxicity profile observed was consistent with the known AEs for the agents being administered.
Any-grade hematologic treatment-related AEs were more common in the palbociclib plus ET arm compared with the chemotherapy arm (96.8% vs 58.6%, respectively). Nonhematologic and treatment-related serious AEs were comparable between treatment arms. One patient death was reported in the palbociclib plus ET arm, caused by septic shock.
PADMA: Conclusion and Takeaways
Heather McArthur, MD, MPH:
As mentioned earlier, the PADMA study met its primary endpoint, showing a statistically significant and clinically meaningful improvement in TTF. Moreover, investigators also reported improvement for the secondary endpoints of PFS and OS. However, OS improvement did not reach statistical significance.
Overall, this outcome is consistent with outcomes of other studies that we have seen in the advanced disease setting where ET together with a CDK4/6 inhibitor have gone head-to-head with chemotherapy, including the RIGHT Choice study evaluating ribociclib with ET vs chemotherapy in premenopausal women with clinically aggressive, HR-positive/HER2-negative ABC.12
The PADMA study has bolstered our confidence in considering ET with CDK4/6 inhibitor therapy even in patients who have high-risk, ER-positive breast cancer, including those with visceral crisis.
RIGHT Choice Subgroup Analysis: First-line Ribociclib Plus ET vs Combination Chemotherapy in Clinically Aggressive HR-Positive/HER2-Negative ABC
Joyce O’Shaughnessy, MD:
In a previous analysis for the phase II RIGHT Choice trial, evaluating ribociclib plus ET vs combination chemotherapy in premenopausal and perimenopausal patients with clinically aggressive ABC, study investigators reported a 9.0-month mPFS benefit in the ITT population with ribociclib plus ET vs combination chemotherapy (mPFS: 21.8 vs 12.8 months, respectively; hazard ratio: 0.61; 95% CI: 0.43-0.87; P = .003).12
At SABCS 2024, we saw an exploratory analysis from RIGHT Choice that evaluated the efficacy of ribociclib plus ET vs combination chemotherapy by PAM50-based intrinsic subtype and gene/signature expression levels in patients with clinically aggressive, HR-positive/HER2-negative ABC.13
RIGHT Choice Subgroup Analysis: Distribution of Patients and PFS by Intrinsic Subtypes
Joyce O’Shaughnessy, MD:
Median PFS in patients with the luminal A subtype was 32.5 months vs not reached (hazard ratio: 0.88) for those receiving ribociclib plus ET vs combination chemotherapy, respectively. Median PFS in patients with the luminal B subtype was 38.0 months vs 21.7 months (hazard ratio: 0.64) for those receiving ribociclib plus ET vs combination chemotherapy, respectively.
We also saw a benefit to ribociclib plus ET vs combination chemotherapy in those with the luminal B/HER2-enriched subtype, often associated with a poor prognosis, with mPFS of 38.0 months vs 18.4 months, respectively (hazard ratio: 0.58).
Of note, the number of patients with visceral crises was comparable in the 2 arms (63.0% vs 68.2%, ribociclib plus ET vs combination chemotherapy, respectively).
RIGHT Choice Subgroup Analysis: PFS by Baseline Gene Expression/Signature Status
Joyce O’Shaughnessy, MD:
Patients with high vs low baseline ESR1 gene expression levels had a longer mPFS (38.0 vs 32.5 months, respectively; hazard ratio: 0.52).
Patients with low expression of tumor inflammatory or immune-related genes/cells such as tumor inflammatory signatures and T-cell expression signatures (ie, at or below the median) had a longer mPFS than patients with high expression of these signatures. By contrast, patients with a higher RB1 gene signature, often associated with a poor prognosis, appear to benefit more with ribociclib plus ET than by receiving treatment with combination chemotherapy.
PFS outcomes by baseline immune-related signatures (eg, B-cell, CD45, CD8 T-cell, and NK cell status) appear to show better outcomes with chemotherapy than with ribociclib plus ET across the various biomarkers evaluated.
RIGHT Choice Subgroup Analysis: Takeaways
Joyce O’Shaughnessy, MD:
With the caveat of small sample sizes, this exploratory analysis of RIGHT Choice showed an mPFS benefit with ribociclib plus ET vs combination chemotherapy in subtypes that are often associated with a poor prognosis (eg, luminal B and luminal B/HER2 enriched).
Ribociclib plus ET is associated with a greater PFS benefit in patients with high vs low baseline ESR1 expression. There was also a more prominent PFS benefit with ribociclib plus ET in patients with low expression of tumor inflammatory or immune-related genes/cells vs those with high expression, and combination chemotherapy was associated with shorter mPFS in patients with low expression of immune-related genes/cells compared with those with high expression.
These data are hypothesis generating regarding the predictive value of intrinsic subtypes and immune-related gene expression levels for assessing the benefit of ribociclib plus ET in patients with clinically aggressive, HR-positive/HER2-negative ABC.
EMBER-3: Imlunestrant With or Without Abemaciclib vs SoC ET in ER-Positive/HER2-Negative ABC After Progression During Prior ET
Heather McArthur, MD, MPH:
At SABCS 2024 we saw the long-awaited results from the international, open-label, randomized phase III EMBER-3 trial of imlunestrant—a next-generation, brain-penetrant, oral, selective estrogen-receptor degrader that delivers continuous ER inhibition—alone or in combination with abemaciclib vs SoC ET (exemestane or fulvestrant). The patients in this trial had ABC or mBC and disease progression during or after AI treatment with or without a CDK4/6 inhibitor in the adjuvant setting or as first-line treatment (N = 874).14,15
The coprimary endpoints of the EMBER-3 study were PFS in the ITT population (imlunestrant vs ET and imlunestrant plus abemaciclib vs imlunestrant) and in patients with ESR1 mutations (confirmed centrally at baseline; imlunestrant vs ET). The secondary endpoints of the study included OS in the ITT population (imlunestrant vs ET and imlunestrant-abemaciclib vs imlunestrant) and in patients with ESR1 mutations (imlunestrant vs ET), ORR, duration of response (DoR), and clinical benefit rate (CBR).
EMBER-3: Baseline Characteristics
Heather McArthur, MD, MPH:
When we look at patients’ baseline characteristics in the EMBER-3 trial, we see that the 3 treatment arms were well balanced. However, there were more patients in the imlunestrant and SoC ET arms than in the imlunestrant-abemaciclib arm. This is because an amendment after the start of the study allowed for the combination of imlunestrant and abemaciclib.
Although there was a modest difference in the proportion of patients with ESR1 mutations enrolled in the imlunestrant arm vs the ET arm vs the imlunestrant-abemaciclib arm (42% vs 36% vs 32%, respectively), we see a very consistent distribution of PIK3CA mutations across the arms (39% vs 39% vs 41%, respectively), and across the treatment arms >50% of patients had visceral metastases. The most common previous CDK4/6 inhibitor received was palbociclib (≥61%).
EMBER-3 PFS for Imlunestrant vs SoC ET (Primary Endpoint)
Heather McArthur, MD, MPH:
The Kaplan-Meier curves show the PFS for imlunestrant vs SoC ET (the primary endpoint). We can see that patients with tumors harboring an ESR1 mutation achieved a significant improvement in their mPFS with imlunestrant vs SoC ET (5.5 vs 3.8 months, respectively; hazard ratio: 0.62; P <.001). However, in the ITT population the improvement in mPFS did not reach statistical significance (5.56 vs 5.5 months, respectively; hazard ratio: 0.87; P <.12).
EMBER-3: PFS for Imlunestrant vs SoC ET by Patient Subgroup
Heather McArthur, MD, MPH:
When we look across the patient subgroups interrogated, with imlunestrant vs SoC ET the numerical benefit achieved is consistent. None of the P values was significant in these subset analyses.
EMBER-3: PFS for Imlunestrant Plus Abemaciclib vs Imlunestrant (Primary Endpoint)
Heather McArthur, MD, MPH:
Looking at the coprimary endpoint of PFS for imlunestrant with abemaciclib vs imlunestrant alone, we see that PFS was 3.9 months longer with imlunestrant plus abemaciclib (9.4 vs 5.5 months, respectively; hazard ratio: 0.57; P <.001). This was almost twice the mPFS with imlunestrant alone.
EMBER-3: PFS for Imlunestrant Plus Abemaciclib vs Imlunestrant in Key Subgroups
Heather McArthur, MD, MPH:
The PFS benefit for imlunestrant with abemaciclib vs imlunestrant alone in key subgroups was also very consistent. Patients who had an ESR1 mutation and received imlunestrant with abemaciclib vs imlunestrant alone benefited the most, with an mPFS of 11.1 months vs 5.5 months, respectively (hazard ratio: 0.53). Overall, all patients benefited from imlunestrant with abemaciclib vs imlunestrant alone, including patients without an ESR1 mutation (mPFS: 9.1 vs 5.5 months, respectively; hazard ratio: 0.59); patients with previous CDK4/6 inhibitor treatment (mPFS: 9.1 vs 3.7 months, respectively; hazard ratio: 0.51); and patients with a PI3K pathway gene mutation (mPFS: 7.6 vs 3.8 months, respectively; hazard ratio: 0.61).
EMBER-3: PFS for Imlunestrant Plus Abemaciclib vs Imlunestrant by Patient Subgroup
Heather McArthur, MD, MPH:
Based on the hazard ratios reported, a consistent benefit was seen across patient subgroups, including those defined by age, number of metastatic sites, visceral metastases, and previous CDK4/6 inhibitor use, all in favor of imlunestrant with abemaciclib vs imlunestrant alone, although the differences were not statistically significant (P >.05).
EMBER-3: Other Efficacy Analyses
Heather McArthur, MD, MPH:
When looking at the results for other efficacy analyses, we can see that the number (rates) of CNS events was lower for patients receiving imlunestrant compared with those who received SoC ET. We also see that there were notable improvements in 6-month and 12-month CNS event rates, as shown in the table on the left, for both the ESR1-mutant population (hazard ratio: 0.18) and in all patients (hazard ratio: 0.47).
EMBER-3: Safety of Imlunestrant vs SoC ET
Heather McArthur, MD, MPH:
The most common (≥10%) treatment-emergent AEs with imlunestrant monotherapy vs SoC ET were fatigue (23% vs 13%), diarrhea (21% vs 12%), and nausea (17% vs 13%).
A similar number of patients receiving imlunestrant monotherapy vs SoC ET experienced ≥1 serious AE (10% vs 12%, respectively). Among those receiving imlunestrant monotherapy, 2% reduced their treatment dose because of an AE; 4% discontinued treatment because of an AE; and 2% were reported to have died during the study because of an AE (vs 1% receiving SoC ET).
EMBER-3 Safety of Imlunestrant Plus Abemaciclib
Heather McArthur, MD, MPH:
The most common (≥20%) any-grade treatment-emergent AEs with imlunestrant plus abemaciclib included diarrhea (86%), nausea (49%), neutropenia (48%), anemia (44%), fatigue (39%), and vomiting (31%). In total, 17% of patients receiving imlunestrant plus abemaciclib experienced ≥1 serious AE; 39% reduced their treatment dose because of an AE; 6% discontinued treatment because of an AE; and 1% were reported to have died during the study because of an AE.
EMBER-3: Takeaways
Heather McArthur, MD, MPH:
My takeaway from the phase III EMBER-3 study is that imlunestrant alone vs SoC ET significantly improved mPFS in patients with ESR1-mutated, HR-positive/HER2-negative ABC, but the same benefit was not observed in the overall ITT population.
What I find most interesting is that the combination of imlunestrant with abemaciclib significantly improved PFS in patients who had HR-positive/HER2-negative ABC irrespective of ESR1 mutation status, and that the benefit was consistent across the subgroups investigated.
Pending an anticipated FDA approval, I believe that the EMBER-3 regimen has become the SoC in the post–CDK4/6 inhibitor plus ET setting in patients with ESR1 mutations, and that the combination of imlunestrant with abemaciclib may potentially become the SoC regardless of ESR1 mutation status.
Joyce O’Shaughnessy, MD:
I agree. In patients with ESR1 mutations, there was a remarkable improvement in PFS, but in the ITT population a significant difference in PFS was not observed. This tells me that imlunestrant is clearly better than fulvestrant and exemestane in the ESR1-mutant population. Regarding imlunestrant with abemaciclib, we saw that the combination was superior to imlunestrant alone in patients with ESR1 mutations, patients with PIK3CA mutations, and patients previously treated with a CDK4/6 inhibitor.
However, in my opinion, I think that the PI3KCA-mutant population would benefit from the triplet combination of fulvestrant, palbociclib, and inavolisib based on the results from the phase III INAVO120 trial in patients with HR-positive/HER2-negative, locally advanced breast cancer or mBC that had relapsed ≤12 months after the completion of adjuvant ET.16,17 However, if those patients are not eligible for inavolisib treatment, meaning their hemoglobin A1C is ≥6%, then we have a choice of using imlunestrant plus abemaciclib or, potentially, fulvestrant plus capivasertib.
ELECTRA and ELEVATE: Elacestrant Combinations for ER-Positive/HER2-Negative ABC/mBC
Joyce O’Shaughnessy, MD:
As already alluded to, after SoC first-line ET plus CDK4/6 inhibition, ER-positive/HER2-negative mBC tumors eventually develop resistance, leading to disease progression.18
Mechanisms of resistance include intrinsic alterations in the PI3K/AKT/mTOR or cell cycle pathway or acquired ESR1 mutations, which are found in up to 50% of patients after initial failure with ET therapy.19-21
Using elacestrant—an FDA-approved,22 oral, selective estrogen receptor degrader for patients with HR-positive/HER2-negative, ESR1-mutated ABC or mBC who have had disease progression after ≥1 previous line of ET—in combination with other PI3K/AKT/mTOR or CDK4/6 inhibitors could potentially help overcome multiple resistance mutations and enable all-oral regimens for patients with refractory/relapsed, ER-positive/HER2-negative mBC tumors.
At SABCS 2024, we saw data on combinations of oral treatments from the ELECTRA and ELEVATE studies. As a reminder, these are international, open-label phase Ib/II dose-escalation and expansion trials in which patients with HR-positive/HER2-negative ABC of any menopausal status were enrolled.23,24
Patients who enrolled in ELECTRA were treated with the combination of elacestrant 258 mg or 345 mg QD and abemaciclib 100 mg or 150 mg BID. These patients had received >1 ET with or without a CDK4/6 inhibitor (excluding abemaciclib) in the advanced setting, and ≤2 lines of previous chemotherapy. The primary endpoints in phase Ib were determining the recommended phase II dose and safety assessment, and in phase II the endpoints were ORR, intracranial response, DoR, CBR, and PFS.
Patients enrolled in ELEVATE received elacestrant 258 mg or 345 mg QD in combination with alpelisib, everolimus, abemaciclib, palbociclib, ribociclib, or capivasertib at varying doses distributed among 3 cohorts in phase Ib and 5 cohorts in phase II. The primary endpoint in phase Ib was the recommended phase II dose and the primary endpoints in phase II included PFS and dose-limiting toxicities.
The analyses presented at SABCS 2024 highlighted safety data and preliminary efficacy data for elacestrant together with abemaciclib in ELECTRA, with updated safety data from additional elacestrant combinations in ELEVATE.
ELECTRA and ELEVATE Pooled Analysis: Baseline Characteristics
Joyce O’Shaughnessy, MD:
The median age for all patients in the pooled study was 60 years, with the median age for those in ELECTRA cohorts 1-3 being between 43 years and 54 years, and for those enrolled in ELEVATE it was 61 years.
Overall, 71% of patients in the pooled analysis had presented with visceral metastases, 53% had ESR1 mutations, and 28% had PIK3CA mutations. The proportion of patients with primary endocrine resistance was 12%.
The median number of lines of therapy in the ELECTRA cohorts 1, 2, and 3 was 2, and for those in ELEVATE it was 1.
ELECTRA and ELEVATE Pooled Analysis: Efficacy
Joyce O’Shaughnessy, MD:
In the table at the top of this slide, one can see that in the ELECTRA cohorts, approximately 30% of patients had experienced a response with elacestrant with abemaciclib, with most of those being partial responses (PRs; 15%-30%). The CBR ranged from 57% to 85%.
The mPFS in all treated patients in ELECTRA was 8.7 months (95% CI: 6.1-16.6 months) and 16.6 months in those who had previously received ET plus a CDK4/6 inhibitor. Median PFS was relatively similar regardless of the dose level. Given the small number of patients in these cohorts, what we can say at this time is that the efficacy for the various combinations appears encouraging.
ELEVATE Update: Safety (Elacestrant Plus Everolimus)
Joyce O’Shaughnessy, MD:
The ELEVATE investigators also looked at the safety profile of the combination of elacestrant and everolimus, an mTOR pathway inhibitor. The most common any-grade AE was nausea, with an incidence of 33% in cohort 2 and up to 75% in cohort 3. Diarrhea and stomatitis were also observed, but those AEs were expected with this combination. Again, with the caveat that these results are in a small number of patients, the safety profile appears consistent with that expected for these agents.
ELEVATE Update: Safety (Elacestrant Plus Palbociclib or Abemaciclib)
Joyce O’Shaughnessy, MD:
We also have updated safety data for the combination of elacestrant with a CDK4/6 inhibitor, in this case either palbociclib or abemaciclib. Again, the toxicity profiles observed are consistent with the known profiles of those individual agents.
Treatment-emergent hematologic AEs of any grade for ELEVATE cohorts 1, 2, and 3 included neutropenia (33%, 67%, and 57%, respectively); decreased platelet counts (17%, 17%, and 29%, respectively); and decreased white blood cells count (0%, 17%, and 29%, respectively).
The most common (all-grade, ≥30%) treatment-emergent AEs with elacestrant 345 mg QD together with abemaciclib 150 mg BID were diarrhea (80%), nausea (63%), fatigue (43%), vomiting (43%), and constipation (30%).
ELEVATE Update: Safety (Elacestrant Plus Ribociclib)
Joyce O’Shaughnessy, MD:
When looking at the safety of elacestrant with another CDK4/6 inhibitor, in this case ribociclib, we saw a very consistent safety profile that is in alignment with the known safety profiles of these 2 agents.
The most common (all-grade, ≥10%) treatment-emergent AEs with elacestrant 258 mg QD together with ribociclib 400 mg QD were vomiting (33%), nausea (17%), fatigue (17%), anemia (17%), and liver enzyme elevation (all 17%).
ELEVATE Update: Safety (Elacestrant Plus Alpelisib or Capivasertib)
Joyce O’Shaughnessy, MD:
We now move on to the combination of elacestrant with the PI3K/AKT pathway inhibitor capivasertib, which is more recently available to us, or alpelisib.
Here the toxicities outlined on the table are primarily grade 1/2. The most common all-grade treatment-emergent AEs with elacestrant plus capivasertib were fatigue (57%), nausea (57%), and vomiting and diarrhea (43% for each). By contrast, with the combination of elacestrant and alpelisib, we saw all-grade treatment-emergent AEs of nausea (~83%-100%), maculopapular rash (33%-50%), and vomiting and fatigue (17%-67%).
ELECTRA and ELEVATE: Takeaways
Joyce O’Shaughnessy, MD:
My takeaway from the ELECTRA and ELEVATE studies is that in patients with ER-positive/HER2-negative ABC who had received previous ET plus a CDK4/6 inhibitor, elacestrant combinations showed consistent safety profiles with promising efficacy.
Again, these are early-stage data from phase I and II studies, but some encouraging activity has been seen, at least in combination with abemaciclib.
DESTINY-Breast06: T-DXd vs Chemotherapy by Pace of Progression During Previous ET in HR-Positive/HER2-Low or HER2-Ultralow mBC
Heather McArthur, MD, MPH:
Patients with HR-positive/HER2-negative mBC face limited treatment options in the second-line setting and beyond. Of importance, approximately 85% of patients with HR-positive/HER2-negative mBC may be classified as HER2 low (based on IHC scores of 1+ or IHC 2+/in situ hybridization–negative) or HER2 ultralow (IHC 0 with faint or incomplete membrane staining in ≤10% of tumor cells).25
Recently we saw the approval of trastuzumab deruxtecan (T-DXd), an anti-HER2 ADC, in patients with HER2-low or HER2-ultralow mBC following disease progression after ≥1 ET, supported by results from the phase III DESTINY-Breast06 trial.26
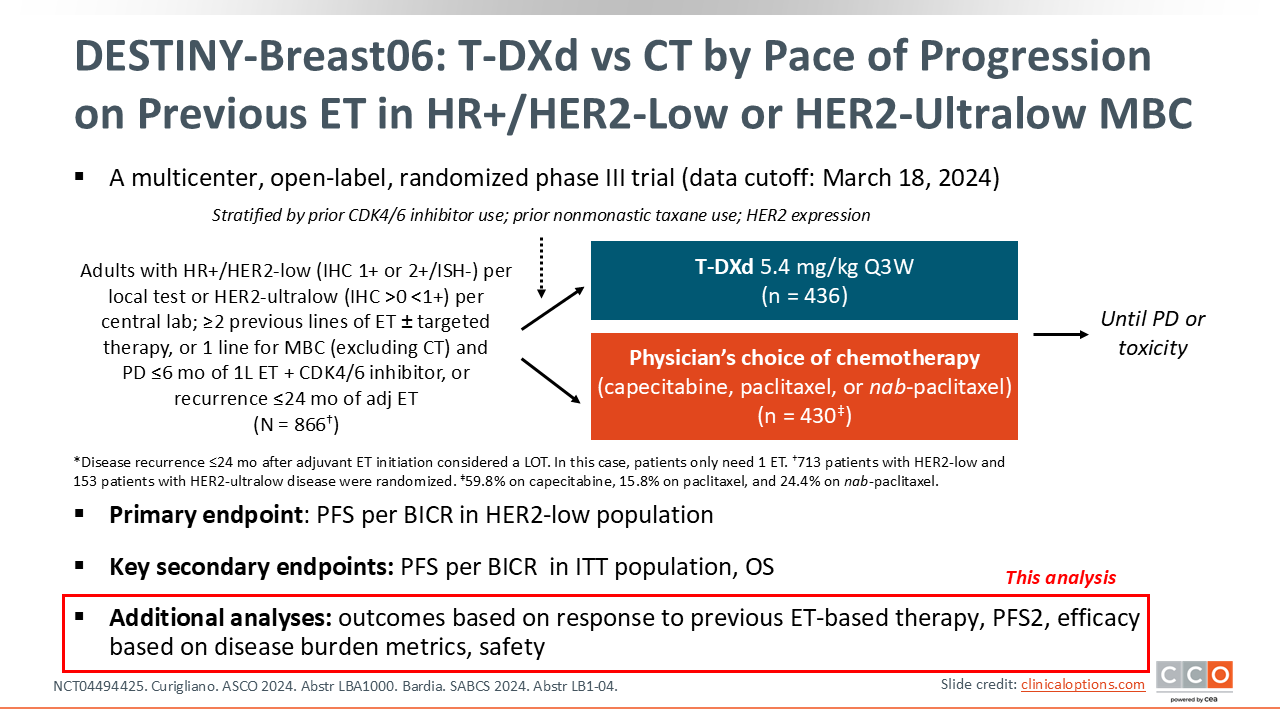
The DESTINY-Breast06 trial is evaluating T-DXd vs physician’s choice of chemotherapy (capecitabine, paclitaxel, or nab-paclitaxel) in patients with HR-positive/HER2-low or HER2-ultralow mBC with disease progression after ET, who had not previously received chemotherapy. The primary endpoint of the study is PFS per blinded independent central review in the HER2-low patient population. The key secondary endpoints include PFS by blinded independent central review in the ITT population and OS.
In a previous report from DESTINY-Breast06, patients receiving T-DXd compared with physician’s choice of chemotherapy achieved statistically significant and clinically meaningful improvement in survival outcomes.27 Median PFS in the HER2-low population was 13.2 months vs 8.1 months, respectively (hazard ratio: 0.62; P <.0001), and in the ITT population (HER2 low plus HER2 ultralow) mPFS was 13.2 months vs 8.1 months, respectively (hazard ratio: 0.64; P <.0001), with numerical OS improvement in favor of T-DXd. OS data were immature.
At SABCS 2024 we saw a report from the DESTINY-Breast06 trial with additional results about the impact of the pace of disease progression during previous ET-based therapy had on outcomes with T-DXd vs physician’s choice of chemotherapy.28
DESTINY-Breast06: Baseline Characteristics
Heather McArthur, MD, MPH:
The median age of patients in the analysis was 58 years. The Eastern Cooperative Oncology Group performance status was ≥1 in 42% of patients; 31% had de novo metastatic disease; and 85% had visceral disease. In total, 31% of patients had primary ET resistance.
DESTINY-Breast06: PFS by TTP During First-line ET Plus CDK4/6 Inhibitor and Endocrine Resistance Status
Heather McArthur, MD, MPH:
Regarding the new results looking at PFS by time to disease progression during first-line ET plus CDK4/6 inhibitor therapy, we see that when compared with chemotherapy of physician’s choice, T-DXd improved mPFS by 7.5 months (mPFS: 14.0 vs 6.5 months, respectively) in patients with disease progression that occurred in <6 months during first-line ET therapy.
An absolute improvement of 6.3 months with T-DXd vs chemotherapy was observed in patients with disease progression that occurred during 6-12 months of first-line ET, and a 4.7-month improvement was seen in those with disease progression after >12 months of first-line ET. Thus, most patients benefited with T-DXd more than with chemotherapy.
Investigators also noted that a PFS benefit was seen regardless of primary ET–resistance status (hazard ratio: 0.57; 95% CI: 0.42-0.77) or secondary ET–resistance status (hazard ratio: 0.68; 95% CI: 0.55-0.84).
Joyce O’Shaughnessy, MD:
I agree with your assessment here. We do see a benefit with T-DXd vs chemotherapy regardless of the time to progression (TTP) during first-line ET and CDK4/6 inhibitor therapy—in other words, regardless of whether patients had a short time or longer time to disease progression with their previous ET.
DESTINY-Breast06: ORR and DoR by TTP During First-line ET Plus CDK4/6 Inhibitor and Endocrine Resistance Status
Heather McArthur, MD, MPH:
Looking at the response rates based on time to disease progression during first-line ET, we see very consistent benefits with T-DXd vs chemotherapy in patients whose disease progressed at <6 months (ORR: 67.7% vs 25.4%, respectively), at 6-12 months (ORR: 60.0% vs 28.8%, respectively), and at >12 months (ORR: 59.5% vs 33.1%, respectively). Similar findings in response rates were noted based on whether patients received T-DXd vs chemotherapy for primary ET resistance (ORR: 57.8% vs 25.7%, respectively) or secondary ET resistance (ORR: 57.1% vs 34.0%, respectively), and across all subgroups analyzed.
DESTINY-Breast06: Time to Second Progression or Death (PFS2) in ITT Population and TTP in Patient Subgroups
Heather McArthur, MD, MPH:
In terms of time from randomization to second progression or death (PFS2), PFS2 delay was clinically meaningful in patients receiving T-DXd vs chemotherapy in the ITT population. Overall, the median PFS2 with T-DXd vs chemotherapy in the ITT population was 20.3 months vs 14.7 months, respectively (hazard ratio: 0.62; P <.0001).
When looking at PFS2 based on TTP, we see a similar trend in improved median PFS2 in patients whose disease had progressed at <6 months (18.9 months with T-DXd vs 15.2 months with chemotherapy; hazard ratio: 0.73); at 6-12 months (17.1 vs 13.7 months, respectively; hazard ratio: 0.59); and at >12 months (20.0 vs 14.3 months, respectively; hazard ratio: 0.57).
DESTINY-Breast06: PFS by Disease Burden
Heather McArthur, MD, MPH:
The study investigators also presented PFS data based on disease burden, and reported that a benefit was seen with T-DXd vs chemotherapy irrespective of disease burden. When looking at patients with liver metastases, in patients with visceral disease, and in patients with baseline tumor size more than the median or less than or equal to the median, we see a very consistent trend of benefit in favor of T-DXd.
DESTINY-Breast06: Safety in TTP and Disease Burden Subgroups
Heather McArthur, MD, MPH:
Overall, T-DXd and chemotherapy safety profiles were comparable to profiles in the overall study population in DESTINY-Breast06 regardless of prior duration of ET and CDK4/6 inhibitor therapy.
Treatment-emergent AEs leading to discontinuation occurred in approximately 14% of patients receiving T-DXd and in 12% of those receiving chemotherapy.
Interstitial lung disease /pneumonitis was experienced by approximately 11% of patients receiving T-DXd and by 0.4% of the patients receiving chemotherapy.
DESTINY-Breast06: Implications and Takeaways
Heather McArthur, MD, MPH:
In this analysis from the phase III DESTINY-Breast06 study, T-DXd was associated with a clinically meaningful PFS benefit compared with chemotherapy in patients with HER2-low and HER2-ultralow mBC, regardless of TTP during first-line ET with a CDK4/6 inhibitor.
These data support our current practice of offering T-DXd to patients with HER2-low and HER2-ultralow disease as opposed to offering chemotherapy, without regard of TTP during their first-line ET.
Joyce O’Shaughnessy, MD:
Another takeaway and implication of this study for me is that T-DXd is a more favorable option for patients who have poor prognostic factors (eg, de novo metastatic disease, liver metastases, visceral disease, and primary ET resistance).
But in my opinion, there was not a subgroup in this study that benefited less than another. This is not surprising with the use of a potent cytotoxic agent such as T-DXd, which clearly outperformed chemotherapy. And last, PFS2 outcomes suggest that T-DXd continues to provide substantial benefits that are sustained beyond that initial delay in disease progression.