CME
Physicians: Maximum of 1.50 AMA PRA Category 1 Credits™
Released: March 04, 2025
Expiration: September 03, 2025
KEYNOTE-522: Biomarker/OS Analyses of Neoadjuvant Pembrolizumab Plus Chemotherapy Followed by Adjuvant Pembrolizumab in TNBC
Joyce O’Shaughnessy, MD:
Previously, investigators for the phase III KEYNOTE-522 trial showed significant improvements in pCR rates, EFS, and OS with neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab when compared with neoadjuvant placebo plus chemotherapy followed by adjuvant placebo in patients with previously untreated, high-risk, early-stage TNBC (T1cN1-2 or T2-4N0-2).31,35,36 At SABCS 2024, we presented a report on the associations among prespecified exploratory biomarkers and pCR and EFS rates, and a report on interim analysis 4 (IA4) together with an analysis of OS in key patient subgroups at interim analysis 7 (IA7).37,38
Exploratory biomarker analysis aimed to assess a relationship between pCR rates and EFS at IA4 (data cutoff: March 23, 2021) with key objectives including TcellinfGEP, TMB, and non-TcellinfGEP consensus signatures. Secondary objectives were to assess TNBC molecular subtypes, homologous recombination deficiency (HRD) status, HER2 gene expression and signature, and PTEN loss signature.
Biomarkers were assessed in tumor biopsies collected at baseline. Whole exome sequencing of tumor tissue and matched blood samples was used to assess TMB, BRCA mutation status, and HRD. RNA sequencing was used to assess tumor tissue for other biomarkers.
KEYNOTE-522 Biomarker Analysis: Association of EFS and pCR With TcellinfGEP and TMB
Joyce O’Shaughnessy, MD:
The study findings showed that TcellinfGEP was positively and significantly associated with higher pCR rates and prolonged EFS irrespective of the treatment used. By contrast, TMB was positively and significantly associated with improved pCR and longer EFS in the pembrolizumab and chemotherapy arm, and TMB was also positively associated with higher pCR but not EFS in the placebo plus chemotherapy arm. I also want to note that HRD was positively associated with pCR but not PFS in both the pembrolizumab and the placebo arms.
KEYNOTE-522 Biomarker Analysis: EFS and pCR With TcellinfGEP and EFS With TMB
Joyce O’Shaughnessy, MD:
Here we have pCR rates and the EFS curves by TcellinfGEP and EFS with TMB. Here again we see that compared with the patients who received placebo plus chemotherapy, those who received pembrolizumab plus chemotherapy experienced an EFS benefit for both the lower level below the first tertile (hazard ratio: 0.68) and the highest level at or above the first tertile (hazard ratio: 0.54) for TcellinfGEP.
Patients whose cancers had high TMB per the prespecified cutoff had a markedly higher EFS rate with pembrolizumab in the TMB subgroup. The pCR rates and hazard ratios for EFS were not examined in the TMB subgroups because the number of patients in the higher TMB subgroup was too small.
KEYNOTE-522 Biomarker Analysis: Associations of EFS and pCR With Non-TcellinfGEP Consensus Signatures
Joyce O’Shaughnessy, MD:
The glycolysis and proliferation signatures were positively associated (1.24 x 10-5 [+]) with pCR and there was a modest inverse association between the stromal epithelial to mesenchymal transition and TGF β signaling with pCR (P = .020 [-]) and EFS (P = .030 [-]) rates in the pembrolizumab plus chemotherapy arm, but not in the placebo plus chemotherapy arm.
A PTEN loss signature was positively associated with pCR rates in both the pembrolizumab arm and placebo arm (4.93 x 10-8 [+] and 6.19 x 10-4 [+], respectively) but EFS was only positively correlated with the pembrolizumab plus chemotherapy arm (P = .017 [+]). And although the presence of HRD correlated with pCR rates in both study arms, there was no correlation with EFS.
KEYNOTE-522 Biomarker Analysis: EFS and pCR in TNBC Molecular Subtypes and Subgroups by HRD Status
Joyce O’Shaughnessy, MD:
The luminal androgen receptor subtype had the lowest pCR rates with chemotherapy plus pembrolizumab but exhibited the largest improvement in pCR rates in patients receiving pembrolizumab plus chemotherapy.
All subtypes saw improved EFS with the addition of pembrolizumab, with the largest absolute benefit in the luminal androgen receptor subgroup (hazard ratio: 0.48; 95% CI: 0.26-0.88). HRD was negatively associated with lower pCR and EFS rates. However, both HRD-positive patients (hazard ratio: 0.67; 95% CI: 0.46-0.96) and HRD-negative patients (hazard ratio: 0.62; 95% CI: 0.33-1.19) experienced improved EFS with the addition of pembrolizumab.
KEYNOTE-522 OS Subgroup Analysis: Objectives and Baseline Characteristics
Joyce O’Shaughnessy, MD:
At SABCS 2024 we also saw results of the OS subgroup analyses from KEYNOTE-522, presented by Dent and colleagues.38
The key objective for these analyses was to assess for efficacy at IA7 for the subgroups by residual cancer burden (RCB); PD-L1 composite positive score (CPS) of ≥10 and <10; overall disease stages II and III; and in patients with positive and negative nodal status. In addition, they did a post hoc analysis of OS in subgroups with baseline T2N0 disease.
In the baseline characteristics specific to the patients evaluated in the subgroup analyses, we see that the arms were relatively well balanced with regard to PD-L1 CPS status, carboplatin schedule, tumor size, nodal involvement, and disease stage (eg, stages II and III).
KEYNOTE-522 Subgroup Analysis: OS in ITT Population and by RCB Status
Joyce O’Shaughnessy, MD:
The addition of pembrolizumab to chemotherapy was shown to improve OS in the ITT population (hazard ratio: 0.66; 95% CI: 0.50-0.87; P = .0015) and in the subgroup of patients with an RCB status of 2 (hazard ratio: 0.66), but not in the RCB-1 and RCB-3 subgroups (hazard ratio: 1.35 and 1.26, respectively). Why no benefit was seen in the RCB-1 or RCB-3 subgroups is open to speculation, but the small number of patients in those groups may have contributed to that result.
KEYNOTE-522 OS Subgroup Analysis: OS by PD-L1 CPS Overall Disease Stage, Nodal Status, and Baseline T2N0 Disease
Joyce O’Shaughnessy, MD:
A numerical OS benefit was also seen in other subgroups including by PD-L1 CPS, overall disease stage, nodal status, and baseline T2N0 disease, with hazard ratios ranging between 0.5 and 0.76.
KEYNOTE-522 Biomarker and OS Subgroups: Takeaways
Joyce O’Shaughnessy, MD:
In the KEYNOTE-522 biomarker subgroups and exploratory analyses we saw that several biomarkers, including TcellinfGEP, were positively prognostic of pCR or EFS, but were not necessarily predictive of benefit with the addition of pembrolizumab to chemotherapy. Of note, TMB was associated with a benefit in the pembrolizumab arm but not the placebo arm.
The most pronounced OS benefit seen in the RCB-2 subgroup, with a positive trend seen by PD-L1 CPS and by T2N0 baseline stage. A key question raised by this study was whether the RCB-0 patients could see a pCR benefit from chemotherapy alone, because this group of patients did relatively well in the pembrolizumab arm and the placebo arm, with 5-year survival rates of approximately 95% in both arms. In addition, exploring more deeply into why some patients with T2N0 respond whereas others do not remains an area of future study.
NSABP B-59/GBG-96-GeparDouze: Neoadjuvant Chemotherapy Plus Atezolizumab Followed by Adjuvant Atezolizumab for Stage II/III TNBC
Joyce O’Shaughnessy, MD:
We also saw data presented for the international, randomized, double-blind phase III GBG-96-GeparDouze trial evaluating neoadjuvant chemotherapy with or without atezolizumab, followed by adjuvant atezolizumab or placebo, in patients with stage II/III TNBC.39 Of note, the chemotherapy backbone consisted of carboplatin and paclitaxel for 12 weeks and cyclophosphamide/doxorubicin or cyclophosphamide/epirubicin for 8-12 weeks, which is similar to what was administered in the KEYNOTE-522 trial.
The primary endpoint for GBG-96-GeparDouze is EFS. Key secondary endpoints include OS, pCR in breast and lymph nodes (ypT0/TisypN0), and safety.
I also want to mention that the use of capecitabine was allowed for those who did not have a pCR, and that was different from the KEYNOTE-522 trial, where capecitabine was not allowed. In addition, patients were allowed to receive olaparib if they had gBRCA-mutated status. This also was not allowed in KEYNOTE-522.
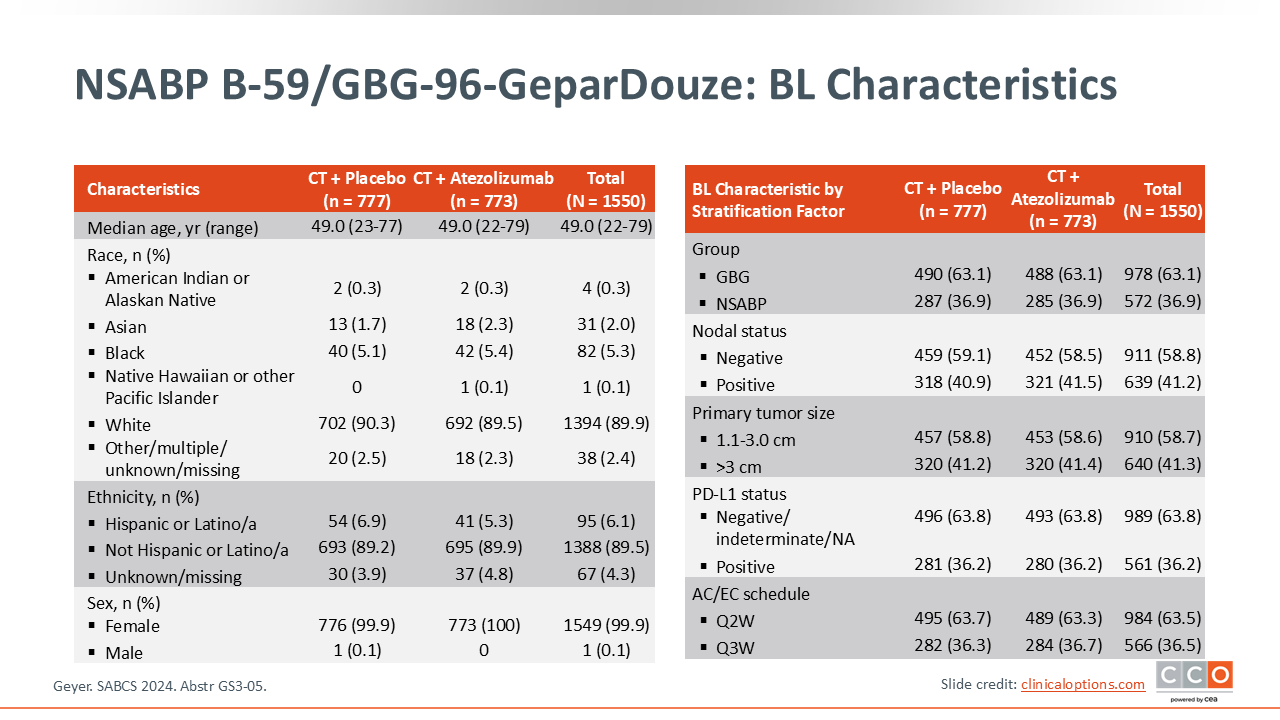
NSABP B-59/GBG-96-GeparDouze: Baseline Characteristics
Joyce O’Shaughnessy, MD:
Regarding patient characteristics, approximately 60% of patients were node negative and approximately the same percentage had a primary tumor size of 1.1-3.0 cm. This contrasts with the KEYNOTE-522 study, in which a higher proportion patients had node-positive disease and tumors >3.0 cm.
Most tumors (94.8%) in GBG-96-GeparDouze were invasive ductal carcinoma; most were grade 3 (~81.0%) or grade 2 disease (~17.7%); and approximately 62% had a tumor-infiltrating lymphocyte level of <30%.
Approximately 53% were wild type for BRCA1/2 and PALB-2, and 36.7% did not have germline testing.
NSABP B-59/GBG-96-GeparDouze: EFS (Primary Endpoint)
Joyce O’Shaughnessy, MD:
Now moving on to the primary endpoint of EFS, after a median follow-up of 46.9 months the study investigators found no difference in EFS between the atezolizumab and placebo control arms (hazard ratio: 0.8; P = .08).
In subgroup analyses, the only patient subgroup with a statistically significant EFS benefit was the subgroup with node-positive status. For every other subgroup analyzed—including by tumor size, PD-L1 status, tumor-infiltrating lymphocyte category, and type of chemotherapy received—there was no statistical difference between the atezolizumab and control arms.
The GBG-96-GeparDouze trial had a lower-risk population than that of the KEYNOTE-522 trial and patients in GBG-96-GeparDouze received other possible treatments, such as olaparib and more chemotherapy, which, in my opinion, may have improved the outcomes for patients on both arms of this trial.
NSABP B-59/GBG-96-GeparDouze: First EFS Events
Joyce O’Shaughnessy, MD:
Most patients had distant recurrences. These occurred slightly more frequent in the placebo arm vs the atezolizumab arm (9.9% vs 7.5%, respectively), with most of them being non-CNS recurrences (6.8% vs 3.8%, respectively).
NSABP B-59/GBG-96-GeparDouze: pCR and OS
Joyce O’Shaughnessy, MD:
The number of patients with a pCR in the breast and lymph nodes was higher in patients receiving atezolizumab vs those receiving placebo, with a statistically significant difference (63.3 vs 57.0, respectively; P = .0091).
After a median follow-up of 46.6 months, the median OS was not reached in either arm and the 4-year OS rates were comparable in the atezolizumab and placebo arms (89.5% and 90.2%, respectively; hazard ratio: 0.86).
NSABP B-59/GBG-96-GeparDouze: Safety Summary and Causes of Death
Joyce O’Shaughnessy, MD:
Regarding treatment-emergent AEs, as expected, some immune-related AEs were observed in the arm containing atezolizumab. Of importance, although treatment had to be discontinued more often because of serious AEs in the atezolizumab arm vs the placebo arm (in 21.2% vs 10.6% of patients, respectively), this did not appear to significantly affect chemotherapy administration or the discontinuation rates caused by AEs for carboplatin/paclitaxel and cyclophosphamide/doxorubicin or cyclophosphamide/epirubicin. In other words, adding atezolizumab to neoadjuvant chemotherapy followed by adjuvant atezolizumab did not adversely affect administration of the chemotherapy planned.
NSABP B-59/GBG-96-GeparDouze: Takeaways
Joyce O’Shaughnessy, MD:
In this phase III study, adding atezolizumab to neoadjuvant chemotherapy followed by adjuvant atezolizumab alone did not statistically significantly prolong EFS. EFS rates at 4 years for the patients receiving atezolizumab and for the patients receiving placebo were 85.2% and 81.9%, respectively, which was not a statistically significant difference (P = .08). On the other hand, adding atezolizumab to neoadjuvant chemotherapy did seem to improve the pCR rate from 57% to 63%, and no new safety signals identified.
This report comes soon after we learned the results of the phase III IMpassion030 trial. That trial looked at adjuvant chemotherapy with or without atezolizumab for patients with resected stage II/III TNBC that was confirmed by central pathology review. The primary endpoint of IMpassion030 was IDFS. At the interim analysis with a median follow-up of approximately 25 months and 239 IDFS events, the hazard ratio for IDFS crossed the prespecified futility boundary.
GBG-96-GeparDouze is a study that adds to the conversation about whether there are differences in checkpoint inhibitors; there are now 2 studies with essentially negative results using atezolizumab in the (neo)adjuvant setting for TNBC.
At this time, the only approved agent in the (neo)adjuvant setting for TNBC is pembrolizumab, in accordance with the phase III KEYNOTE-522 study.40
Again, key differences of the GBG-96-GeparDouze trial vs the KEYNOTE-522 trial included trial size and that KEYNOTE-522 had coprimary endpoints of pCR and EFS, whereas GBG-96-GeparDouze had only the one primary endpoint of EFS. Thus, GBG-96-GeparDouze was more modestly powered. It is also possible that failure to meet the primary endpoint of showing an EFS difference in GBG-96-GeparDouze was a function of the study sample size and the additional treatments given. Based on these results, at this time we do not expect atezolizumab to be moving forward in the early-stage TNBC (neo)adjuvant setting.